Improved Blood Biomarkers but No Cognitive Effects from 16 Weeks of Multivitamin Supplementation in Healthy Older Adults

Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Multivitamin Supplements and Placebo

{kind=link}
| Ingredient | Women’s | RDI Women | Men’s | RDI Men |
|---|---|---|---|---|
| Retinyl Acetate | 862.5 μg | 700 μg | 862.5 μg | 900 μg |
| d-Alpha-Tocopheryl Acid Succinate | 20 mg | 7 mg | 25 mg | 10 mg |
| Thiamine Hydrochloride (vitamin B1) | 30 mg | 1.1 mg | 35 mg | 1.2 mg |
| Riboflavine (vitamin B2) | 30 mg | 1.1 mg | 35 mg | 1.3 mg |
| Nicotinamide (vitamin B3) | 20 mg | 14 mg | 25 mg | 16 mg |
| Calcium Pantothenate (vitamin B5) | 70 mg | 4 mg | 75 mg | 6 mg |
| Pyrodoxine Hydrochloride (vitamin B6) | 30 mg | 1.5 mg | 25 mg | 1.7 mg |
| Cyanocobalamin (vitamin B12) | 115 μg | 2.4 μg | 120 μg | 2.4 μg |
| Cholecalciferol (vitamin D3) | 5 μg | 10 μg | 5 μg | 10 μg |
| Biotin (vitamin H) | 150 μg | 25 μg | 200 μg | 30 μg |
| Folic Acid | 500 μg | 400 μg | 500 μg | 400 μg |
| Calcium Ascorbate Dihydrate (vitamin C) | 200 mg | 45 mg | 200 mg | 45 mg |
| Phytomedadione (vitamin K1) | 60 μg | 60 μg | 70 μg | 70 μg |
| Calcium Orotate | 100 mg | 1000 mg | 100 mg | 1300 mg |
| Magnesium Aspartate Dihydrate | 100 mg | 320 mg | 100 mg | 420 mg |
| Selenomethionine | 65 μg | 60 μg | 65 μg | 70 μg |
| Molybdenum Trioxide | 67.5 μg | 45 μg | 67.5 μg | 45 μg |
| Chromium Picolinate | 402 μg | 25 μg * | 402 μg | 35 μg * |
| Manganese Amino Acid Chelate | 30 mg | 5 mg | 40 mg | 5.5 mg |
| Ferrous Fumarate | 16.01 mg | 8 mg | 16.01 mg | 8 mg |
| Copper Gluconate | 8.57 mg | 1.2 mg * | 12.14 mg | 1.7 mg * |
| Potassium Iodide | 196 μg | 150 μg 2800 mg * | 196 μg | 150 μg 3800 mg * |
| Zinc Amino Acid Chelate | 75 mg | 8 mg | 100 mg | 14 mg |
| Ingredient | Women’s | Men’s | ||
| Lactobacillus rhamnosus | 80 million organisms | 80 million organisms | ||
| Lactobacillus acidophilus | 80 million organisms | 80 million organisms | ||
| Bifidobacterium longum | 35 million organisms | 35 million organisms | ||
| Vaccinium Macrocarpon Fruit Dry (patented cranberry PACRAN) | 800 mg | 1000 mg | ||
| Citrus Bioflavoloids Extract | 20 mg | 20 mg | ||
| Silybum Marianum Dry Fruit (St. Mary’s thistle) | 1500 mg | 1700 mg | ||
| Ginkgo Biloba Leaf Dry | 1000 mg | 1000 mg | ||
| Crataegus Monogyna Fruit Dry (Hawthorn) | 100 mg | 120 mg | ||
| Cynara Scolymus Leaf Dry (Globe artichoke) | 50 mg | 50 mg | ||
| Lecithin Powder—Soy Phosphatidylserine Enriched Soy | 10 mg | 10 mg | ||
| Scutellaria Lateriflora Herb Dry (Skullcap) | 50 mg | 50 mg | ||
| Spearmint Oil | 2 mg | 2 mg | ||
| Tagetes Erecta Flower Dry (Marigold) | 100 mg | 100 mg | ||
| Ubidecarenone (Co-enzyme Q10) (from patented Ultrasome CoQ10) | 2 mg | 3 mg | ||
| Urtica Dioica Leaf Dry (Nettle) | 100 mg | 50 mg | ||
| Vaccinium Myrtillus Fruit Dry (Bilberry) | 100 mg | 100 mg | ||
| Vitis Vinifera Dry Seed (Grape seed) | 1000 mg | 1000 mg | ||
| Bacopa Monnieri Whole Plant Dry | 50 mg | - | ||
| Cimifuga Racemosa Root & Rhizome Dry (Black cohosh) | 200 mg | - | ||
| Curcuma Longa Rhizome Dry (Turmeric) | 100 mg | - | ||
| Silica Colloidal Anhydrous | 20 mg | - | ||
| Tunera Diffusa Leaf Dry (Damiana) | 500 mg | - | ||
| Withania Somnifera Root Dry (Ashwagandha) | 500 mg | - | ||
| Dulacia Inopiflora Root Dry (Muirapuama) | - | 200 mg | ||
| Serenoa Repens Fruit Dry (Saw palmetto) | - | 300 mg | ||
| Tribulus Terrestris Fruit & Root Dry (Tribulus) | - | 1000 mg |
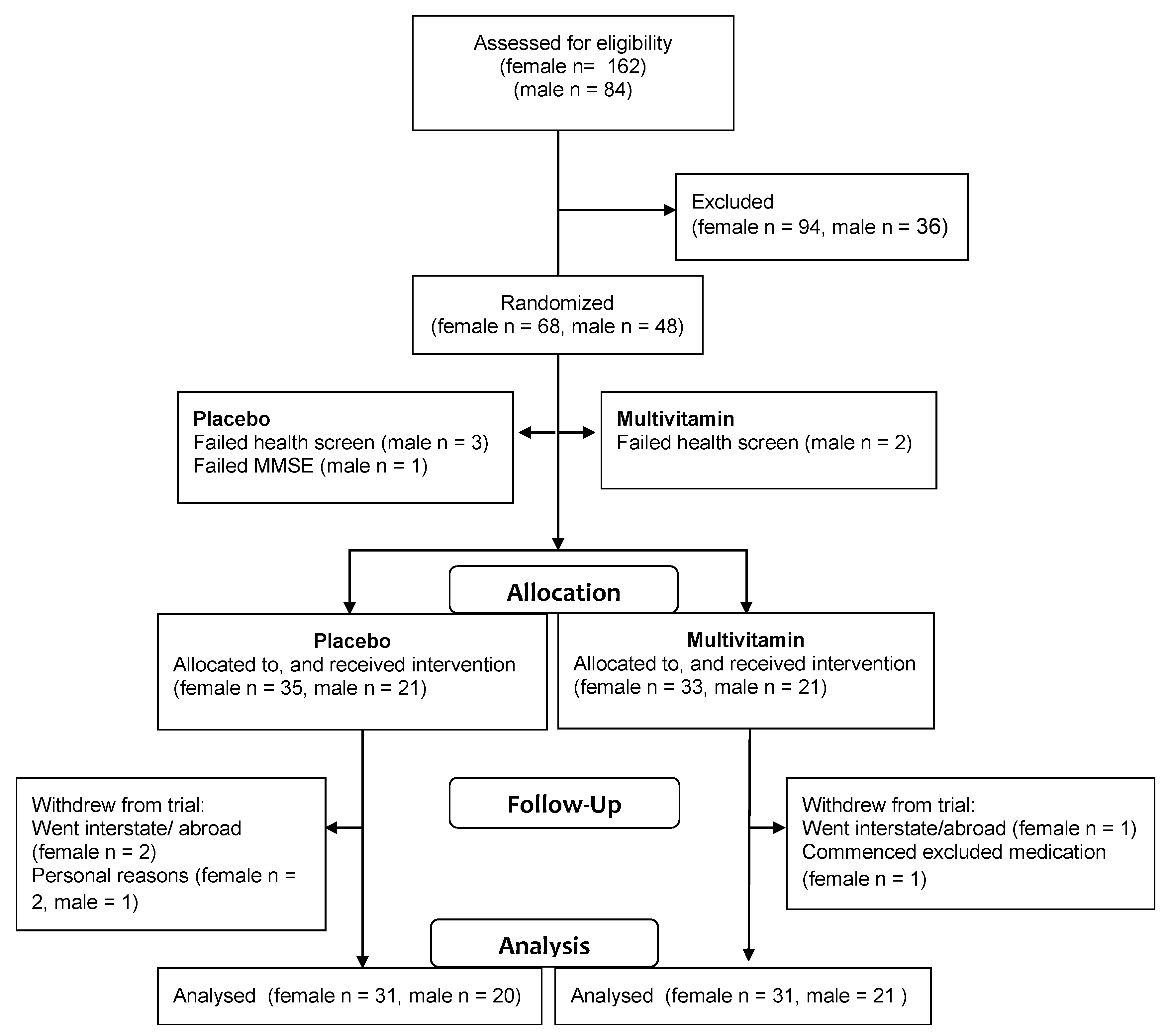
2.3. Sample Size Calculation and Randomisation
2.4. Measures and Procedures
2.5. Statistical Analysis
3. Results
| Characteristic | Placebo Multivitamin | ||||
|---|---|---|---|---|---|
| M (SD) | Range | M (SD) | Range | p | |
| Males | |||||
| Age—years | 59.1 (2.3) | 55–65 | 60.2 (3.2) | 55–65 | 0.214 |
| Education—years | 16.5 (3.8) | 11–27 | 16.0 (3.9) | 11–23 | 0.602 |
| BMI—kg/m2 | 26.8 (2.9) | 21.4–32.3 | 26.8 (6.2) | 19.0–49.2 | 0.138 |
| Females | |||||
| Age—years | 60.1 (3.4) | 54–65 | 60.2 (3.2) | 55–65 | 0.818 |
| Education—years | 14.7 (3.8) | 9–24 | 16.0 (3.9) | 11–23 | 0.163 |
| BMI—kg/m2 | 26.3 (4.4) | 18.5–36.5 | 26.8 (6.2) | 19.0–49.1 | 0.717 |

3.1. Cognitive Test Results—Women’s and Men’s Formulas
3.2. Blood Test Results—Women’s Formula
| Females | Males | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Post | n | Baseline | Post | n | ||
| M (SD) | M (SD) | M (SD) | M (SD) | ||||
| Spatial Mem., % | PL | 67.1 (13.8) | 70.5 (10.6) | 30 | 78.1 (9.9) | 81.5 (9.2) | 16 |
| MV | 68.7 (13.2) | 71.4 (13.3) | 26 | 74.9 (16.1) | 77.0 (15.7) | 21 | |
| Spatial Mem., ms | PL | 1200 (190) | 1132 (127) | 30 | 1023 (136) | 996 (115) | 16 |
| MV | 1146 (166) | 1099 (161) | 26 | 1018 (181) | 975 (183) | 21 | |
| Contextual, % | PL | 74.3 (17) | 73.2 (11.7) | 28 | 69.7 (13.0) | 63.8 (12.5) | 16 |
| MV | 78.5 (13) | 71.1 (13.0) | 27 | 73.4 (17.7) | 64.2 (16.9) | 19 | |
| Contextual, ms | PL | 1130 (157) | 1081 (135) | 29 | 1069 (131) | 1082 (116) | 16 |
| MV | 1070 (123) | 1073 (139) | 27 | 1077 (135) | 1061 (168) | 19 | |
| Stroop Interfere., ms | PL | 205 (134) | 217 (142) | 27 | 220 (207) | 152 (109) | 15 |
| MV | 187 (135) | 188 (139) | 23 | 121 (94) | 132 (80) | 17 | |
| Stroop Congruent, ms | PL | 775 (91.6) | 784 (88) | 29 | 746 (81) | 780 (95) | 16 |
| MV | 776 (109) | 745 (93) | 27 | 743 (99) | 726 (102) | 21 | |
| Stroop Incong., % | PL | 94.1 (6.2) | 93.7 (9.7) | 28 | 91.5 (15.3) | 93.2 (7.6) | 15 |
| MV | 94.0 (11.4) | 94.9 (6.0) | 23 | 97.8 (3.4) | 97.5 (4.2) | 17 | |
| Stroop Incong., ms | PL | 979 (148) | 1000 (140) | 28 | 970 (165) | 938 (106) | 15 |
| MV | 941 (185) | 919 (177) | 23 | 851 (127) | 854 (99) | 17 | |
| Simple RT, ms | PL | 278 (27.1) | 274 (33) | 27 | 262 (32) | 257 (27) | 17 |
| MV | 276 (26.8) | 272 (29) | 25 | 260 (24) | 258 (17) | 20 | |
| Choice RT, ms | PL | 491 (61) | 485 (58) | 27 | 462 (42) | 488 (63) | 17 |
| MV | 499 (66) | 501 (65) | 27 | 467 (56) | 457 (50) | 20 | |
| Immed. Recog., % | PL | 67.4 (11.7) | 76.4 (9.0) | 28 | 70.7 (12.0) | 79.8 (7.6) | 15 |
| MV | 70.3 (13.0) | 78.2 (8.0) | 24 | 67.0 (12.2) | 76.7 (8.7) | 20 | |
| Immed. Recog., ms | PL | 1151 (161) | 1087 (133) | 28 | 1129 (174) | 1095 (160) | 15 |
| MV | 1084 (102) | 1054 (127) | 24 | 1144 (153) | 1060 (179) | 20 | |
| Delayed Recog., % | PL | 68.0 (8.7) | 75.2 (10.4) | 28 | 66.0 (14.3) | 70.5 (7.6) | 14 |
| MV | 71.2 (9.4) | 73.6 (12.3) | 26 | 69.0 (10.0) | 70.7 (14.0) | 20 | |
| Delayed Recog., ms | PL | 1064 (141) | 1020 (126) | 28 | 1123 (162) | 1081 (155) | 14 |
| MV | 1077 (128) | 1023 (148) | 26 | 1073 (95) | 1014 (147) | 19 | |
| Test Units | Females | Males | |||||
|---|---|---|---|---|---|---|---|
| Baseline | Post-Treatment | n | Baseline | Post-Treatment | n | ||
| M (SD) | M (SD) | M (SD) | M (SD) | ||||
| Homocysteine, µmol/L | PL | 13.0 (2.9) | 14.4 (3.9) | 31 ‡ | 15.5 (3.9) | 16.2 (3.2) | 17 † |
| MV | 12.9 (3.0) | 12.6 (2.5) | 28 | 15.1 (3.4) | 13.7 (2.8) | 21 | |
| Vitamin B12, pmol/L | PL | 300 (78) | 298 (91) | 31 * | 284 (100) | 249 (84) | 15 * |
| MV | 300 (103) | 435 (143) | 28 | 265 (63) | 342 (120) | 19 | |
| Vitamin B6, nmol/L | PL | 88 (28) | 118 (92) | 28 * | 151 (120) | 160 (155) | 13 * |
| MV | 104 (53) | 467 (215) | 23 | 121 (89) | 335 (134) | 15 | |
| Folate, nmol/L | PL | 744 (290) | 800 (228) | 30 | 601 (187) | 614 (156) | 17 |
| MV | 922 (180) | 933 (309) | 28 | 683 (298) | 793 (303) | 19 | |
| CRP, mg/L | PL | 1.9 (2.2) | 1.8 (2.1) | 27 † | 1.4 (1.5) | 0.9 (0.9) | 15 |
| MV | 1.9 (2.5) | 1.1 (1.2) | 24 | 1.9 (1.7) | 1.1 (0.8) | 20 | |
| Fibrinogen, g/L | PL | 3.1 (0.3) | 3.0 (0.4) | 30 | 3.0 (0.6) | 3.1 (0.3) | 14 |
| MV | 3.0 (0.5) | 3.0 (0.5) | 26 | 2.9 (0.4) | 2.9 (0.5) | 20 | |
| Prot Carbonyl, mol/mL | PL | 19.6 (7.1) | 17.6 (3.5) | 24 | 19.1 (5.2) | 19.4 (4.5) | 15 |
| MV | 18.2 (7.05) | 19.0 (5.1) | 24 | 20.5 (5.1) | 16.4 (4.6) | 15 | |
| Total Chol, mmol/L | PL | 6.0 (1.1) | 5.8 (0.9) | 31 | 5.6 (0.9) | 5.7 (1.1) | 17 |
| MV | 5.7 (0.8) | 5.8 (0.8) | 29 | 5.6 (0.7) | 5.3 (0.9) | 21 | |
| HDL, mmol/L | PL | 1.80 (0.40) | 1.88 (0.48) | 31 | 1.54 (0.30) | 1.52 (0.36) | 17 |
| MV | 1.90 (0.38) | 2.07 (0.56) | 29 | 1.51 (0.42) | 1.46 (0.39) | 20 | |
| LDL, mmol/L | PL | 3.70 (0.97) | 3.40 (1.05) | 31 | 3.42 (0.67) | 3.44 (0.79) | 17 ‡ |
| MV | 3.37 (0.66) | 3.11 (0.96) | 29 | 3.45 (0.59) | 3.06 (0.89) | 20 | |
| Triglyceride, mmol/L | PL | 1.2 (0.5) | 1.2 (0.6) | 31 | 1.2 (0.5) | 1.4 (0.6) | 16 |
| MV | 1.0 (0.4) | 1.1 (0.4) | 28 | 1.3 (0.5) | 1.4 (0.6) | 21 | |
| LDL/HDL ratio | PL | 2.2 (0.7) | 2.1 (0.7) | 31 | 2.3 (0.6) | 2.2 (0.7) | 17 |
| MV | 1.8 (0.5) | 1.8 (0.5) | 29 | 2.5 (0.7) | 2.3 (0.5) | 21 | |
| Chol/HDL ratio | PL | 3.5 (0.9) | 3.4 (0.8) | 31 | 3.7 (0.7) | 3.8 (0.8) | 17 ‡ |
| MV | 3.1 (0.6) | 3.1 (0.6) | 29 | 4.0 (0.9) | 3.8 (0.7) | 21 | |
| AST, U/L | PL | 23.0 (5.7) | 21.3 (5.3) | 29 * | 24.2 (6.0) | 24.0 (7.1) | 16 |
| MV | 21.4 (45.0) | 26.2 (9.7) | 29 | 23.1 (6.2) | 25.0 (5.9) | 21 | |
| ALT, U/L | PL | 22.9 (10.1) | 20.9 (9.1) | 29 * | 27.5 (12.2) | 27.6 (9.4) | 16 |
| MV | 18.1 (4.0) | 22.9 (5.4) | 27 | 25.6 (7.9) | 30.5 (9.9) | 21 | |
3.3. Blood Test Results—Men’s Formula
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Gillette-Guyonnet, S.; van Kan, A.G.; Andrieu, S.; Barberger-Gateau, P.; Berr, C.; Bonnefoy, M.; Dartigues, J.F.; de Groot, L.; Ferry, M.; Galan, P.; et al. Iana task force on nutrition and cognitive decline with aging. J. Nutr. Health Aging 2007, 11, 132–152. [Google Scholar] [PubMed]
- Kennedy, D.O.; Haskell, C.F. Vitamins and cognition: What is the evidence? Drugs 2011, 71, 1957–1971. [Google Scholar] [CrossRef] [PubMed]
- Ahlemeyer, B.; Krieglstein, J. Neuroprotective effects of ginkgo biloba extract. Cell. Mol. Life Sci. 2003, 60, 1779–1792. [Google Scholar] [CrossRef] [PubMed]
- Gohil, K.J.; Patel, J.J. A review on bacopa monniera: Current research and future prospects. Int. J. Green Pharm. 2010, 4, 1–9. [Google Scholar] [CrossRef]
- NHMRC. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; National Health and Medical Research Council, Australian Government Department of Health and Ageing: Canberra, ACT, Australia, 2006. [Google Scholar]
- Bender, D.A. Nutritional Biochemistry of the Vitamins; Cambridge University Press: New York, NY, USA, 2003. [Google Scholar]
- Benton, D. To establish the parameters of optimal nutrition do we need to consider psychological in addition to physiological parameters? Mol. Nutr. Food Res. 2013, 57, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Wahlqvist, M.L.; Tienboon, P. Growth and ageing. In Nutrition and Metabolism, 2nd ed.; Lanham-New, S.A., Macdonald, I.A., Eds.; John Wiley & Sons Ltd.: West Sussex, UK, 2011. [Google Scholar]
- Prins, N.D.; den Heijer, T.; Hofman, A.; Koudstaal, P.J.; Jolles, J.; Clarke, R.; Breteler, M.M.B. Homocysteine and cognitive function in the elderly: The rotterdam scan study. Neurology 2002, 59, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.J. Homocysteine-lowering trials for prevention of cardiovascular events: A review of the design and power of the large randomized trials. Am. Heart J. 2006, 151, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.K.; Saxby, B.K.; Firbank, M.J.; O’Brien, J.T.; Harrington, F.; McKeith, I.G.; Hansrani, M.; Stansby, G.; Ford, G.A. Plasma homocysteine and cognitive decline in older hypertensive subjects. Int. Psychogeriatr. 2011, 23, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; van Boxtel, M.P.J.; Bosma, H.; Bosmans, E.; Delanghe, J.; de Bruijn, C.; Wauters, A.; Maes, M.; Jolles, J.; Steinbusch, H.W.M.; et al. Inflammation markers in relation to cognition in a healthy aging population. J. Neuroimmunol. 2003, 134, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Engelhart, M.J.; Geerlings, M.I.; Meijer, J.; Kiliaan, A.; Ruitenberg, A.; van Swieten, J.C.; Stijnen, T.; Hofman, A.; Witteman, J.C.M.; Breteler, M.M.B.; et al. Inflammatory proteins in plasma and the risk of dementia: The rotterdam study. Arch. Neurol. 2004, 61, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Murphy, E.A.; Carmichael, M.D. Effects of the dietary flavonoid quercetin upon performance and health. Curr. Sports Med. Rep. 2009, 8, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Shab-Bidar, S.; Neyestani, T.R.; Djazayery, A.; Eshraghian, M.R.; Houshiarrad, A.; Kalayi, A.; Shariatzadeh, N.; Khalaji, N.; Gharavi, A. Improvement of vitamin D status resulted in amelioration of biomarkers of systemic inflammation in the subjects with type 2 diabetes. Diabetes/Metab. Res. Rev. 2012, 28, 424–430. [Google Scholar] [CrossRef]
- Morris, M.S.; Sakakeeny, L.; Jacques, P.F.; Picciano, M.F.; Selhub, J. Vitamin B-6 intake is inversely related to, and the requirement is affected by, inflammation status. J. Nutr. 2010, 140, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Lai, C.Q.; Mattei, J.; Ordovas, J.M.; Tucker, K.L. Association of vitamin B-6 status with inflammation, oxidative stress, and chronic inflammatory conditions: The boston puerto rican health study. Am. J. Clin. Nutr. 2010, 91, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Barja, G. Free radicals and aging. Trends Neurosci. 2004, 27, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Chin, S.F.; Ibahim, J.; Makpol, S.; Abdul Hamid, N.A.; Abdul Latiff, A.; Zakaria, Z.; Mazlan, M.; Mohd Yusof, Y.A.; Abdul Karim, A.; wan Ngah, W.Z.; et al. Tocotrienol rich fraction supplementation improved lipid profile and oxidative status in healthy older adults: A randomized controlled study. Nutr. Metab. 2011, 8. [Google Scholar] [CrossRef]
- Young, J.M.; Shand, B.I.; McGregor, P.M.; Scott, R.S.; Frampton, C.M. Comparative effects of enzogenol® and vitamin C supplementation versus vitamin C alone on endothelial function and biochemical markers of oxidative stress and inflammation in chronic smokers. Free Radic. Res. 2006, 40, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Gillette-Guyonnet, S.; Secher, M.; Vellas, B. Nutrition and neurodegeneration: Epidemiological evidence and challenges for future research. Br. J. Clin. Pharmacol. 2013, 75, 738–755. [Google Scholar] [PubMed]
- Harris, E.; MacPherson, H.; Vitetta, L.; Kirk, J.; Sali, A.; Pipingas, A. Effects of a multivitamin, mineral and herbal supplement on cognition and blood biomarkers in older men: A randomised, placebo-controlled trial. Hum. Psychopharmacol. 2012, 27, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Summers, W.K.; Martin, R.L.; Cunningham, M.; Deboynton, V.L.; Marsh, G.M. Complex antioxidant blend improves memory in community-dwelling seniors. J. Alzheimer’s Dis. 2010, 19, 429–439. [Google Scholar]
- Kesse-Guyot, E.; Fezeu, L.; Jeandel, C.; Ferry, M.; Andreeva, V.; Amieva, H.; Hercberg, S.; Galan, P. French adults’ cognitive performance after daily supplementation with antioxidant vitamins and minerals at nutritional doses: A post hoc analysis of the supplementation in vitamins and mineral antioxidants (su.Vi.Max) trial. Am. J. Clin. Nutr. 2011, 94, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Grodstein, F.; Kang, J.H.; Glynn, R.J.; Cook, N.R.; Gaziano, J.M. A randomized trial of beta carotene supplementation and cognitive function in men: The physicians’ health study ii. Arch. Intern. Med. 2007, 167, 2184–2190. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.H.; Almeida, O.P. Effect of homocysteine lowering treatment on cognitive function: A systematic review and meta-analysis of randomized controlled trials. J. Alzheimer's Dis. 2012, 29, 133–149. [Google Scholar]
- Kang, J.H.; Cook, N.; Manson, J.; Buring, J.E.; Grodstein, F. A randomized trial of vitamin E supplementation and cognitive function in women. Arch. Intern. Med. 2006, 166, 2462–2468. [Google Scholar] [CrossRef] [PubMed]
- Trabetti, E. Homocysteine, MTHFR gene polymorphisms, and cardio-cerebrovascular risk. J. Appl. Genet. 2008, 49, 267–282. [Google Scholar] [CrossRef] [PubMed]
- Pipingas, A.; Harris, E.; Tournier, E.; King, R.; Kras, M.; Stough, C.K. Assessing the efficacy of nutraceutical interventions on cognitive functioning in the elderly. Curr. Top. Nutraceutical Res. 2010, 8, 79–87. [Google Scholar]
- MacPherson, H.; Ellis, K.A.; Sali, A.; Pipingas, A. Memory improvements in elderly women following 16 weeks treatment with a combined multivitamin, mineral and herbal supplement a randomized controlled trial. Psychopharmacology 2012, 220, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Pipingas, A.; Silberstein, R.B.; Vitetta, L.; van Rooy, C.; Harris, E.V.; Young, J.M.; Frampton, C.M.; Sali, A.; Nastasi, J. Improved cognitive performance after dietary supplementation with a pinus radiata bark extract formulation. Phytother. Res. 2008, 22, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Carobene, A.; Braga, F.; Roraas, T.; Sandberg, S.; Bartlett, W.A. A systematic review of data on biological variation for alanine aminotransferase, aspartate aminotransferase and γ-glutamyl transferase. Clin. Chem. Lab. Med. 2013, 51, 1997–2007. [Google Scholar] [CrossRef] [PubMed]
- Wouters-Wesseling, W.; Wagenaar, L.W.; Rozendaal, M.; Deijen, J.B.; de Groot, L.C.; Bindels, J.G.; van Staveren, W.A. Effect of an enriched drink on cognitive function in frail elderly persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 265–270. [Google Scholar] [CrossRef]
- Davies, K.J. Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. IUBMB Life 2000, 50, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.M.; Ryan, M.C.; Boyle, A.J. The novel role of C-reactive protein in cardiovascular disease: Risk marker or pathogen. Int. J. Cardiol. 2006, 106, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.K.; Yen, C.J.; Chang, C.H.; Kuo, C.K.; Chen, J.H.; Sorond, F. Relation of C-reactive protein to stroke, cognitive disorders, and depression in the general population: Systematic review and meta-analysis. Lancet Neurol. 2005, 4, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Scheurig, A.C.; Thorand, B.; Fischer, B.; Heier, M.; Koenig, W. Association between the intake of vitamins and trace elements from supplements and C-reactive protein: Results of the monica/kora augsburg study. Eur. J. Clin. Nutr. 2008, 62, 127–137. [Google Scholar] [CrossRef]
- Doran, B.; Zhu, W.; Muennig, P. Gender differences in cardiovascular mortality by C-reactive protein level in the united states: Evidence from the national health and nutrition examination survey iii. Am. Heart J. 2013, 166, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R. Lowering blood homocysteine with folic acid based supplements: Meta-Analysis of randomised trials. Br. Med. J. 1998, 316, 894–898. [Google Scholar] [CrossRef]
- De Jager, C.A.; Oulhaj, A.; Jacoby, R.; Refsum, H.; Smith, A.D. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2012, 27, 592–600. [Google Scholar]
- Marian, M.; Sacks, G. Invited review: Micronutrients and older adults. Nutr. Clin. Pract. 2009, 24, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Dragsted, L.O.; Pedersen, A.; Hermetter, A.; Basu, S.; Hansen, M.; Haren, G.R.; Kall, M.; Breinholt, V.; Castenmiller, J.J.M.; Stagsted, J.; et al. The 6-a-day study: Effects of fruit and vegetables on markers of oxidative stress and antioxidative defense in healthy nonsmokers. Am. J. Clin. Nutr. 2004, 79, 1060–1072. [Google Scholar] [PubMed]
- Peng, J.; Jones, G.L.; Watson, K. Stress proteins as biomarkers of oxidative stress: Effects of antioxidant supplements. Free Radic. Biol. Med. 2000, 28, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Karajibani, M.; Montazerifar, F.; Hashemi, M.; Bolour, A.; Dikshit, M. Effects of antioxidant vitamin supplements on lipid profiles and antioxidant capacity in cardiovascular patients. Rawal Med. J. 2011, 36, 251–254. [Google Scholar]
- Gunasekara, P.; Hettiarachchi, M.; Liyanage, C.; Lekamwasam, S. Effects of zinc and multimineral vitamin supplementation on glycemic and lipid control in adult diabetes. Diabetes Metab. Syndr. Obes. Targets Ther. 2011, 4, 53–60. [Google Scholar]
- Huang, J.; Frohlich, J.; Ignaszewski, A.P. The impact of dietary changes and dietary supplements on lipid profile. Can. J. Cardiol. 2011, 27, 488–505. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harris, E.; Macpherson, H.; Pipingas, A. Improved Blood Biomarkers but No Cognitive Effects from 16 Weeks of Multivitamin Supplementation in Healthy Older Adults. Nutrients 2015, 7, 3796-3812. https://doi.org/10.3390/nu7053796
Harris E, Macpherson H, Pipingas A. Improved Blood Biomarkers but No Cognitive Effects from 16 Weeks of Multivitamin Supplementation in Healthy Older Adults. Nutrients. 2015; 7(5):3796-3812. https://doi.org/10.3390/nu7053796
Chicago/Turabian StyleHarris, Elizabeth, Helen Macpherson, and Andrew Pipingas. 2015. "Improved Blood Biomarkers but No Cognitive Effects from 16 Weeks of Multivitamin Supplementation in Healthy Older Adults" Nutrients 7, no. 5: 3796-3812. https://doi.org/10.3390/nu7053796