Randomized Controlled Trial Examining the Effects of Fish Oil and Multivitamin Supplementation on the Incorporation of n-3 and n-6 Fatty Acids into Red Blood Cells

Abstract
:1. Introduction
2. Methods
2.1. Participants

2.2. Setting
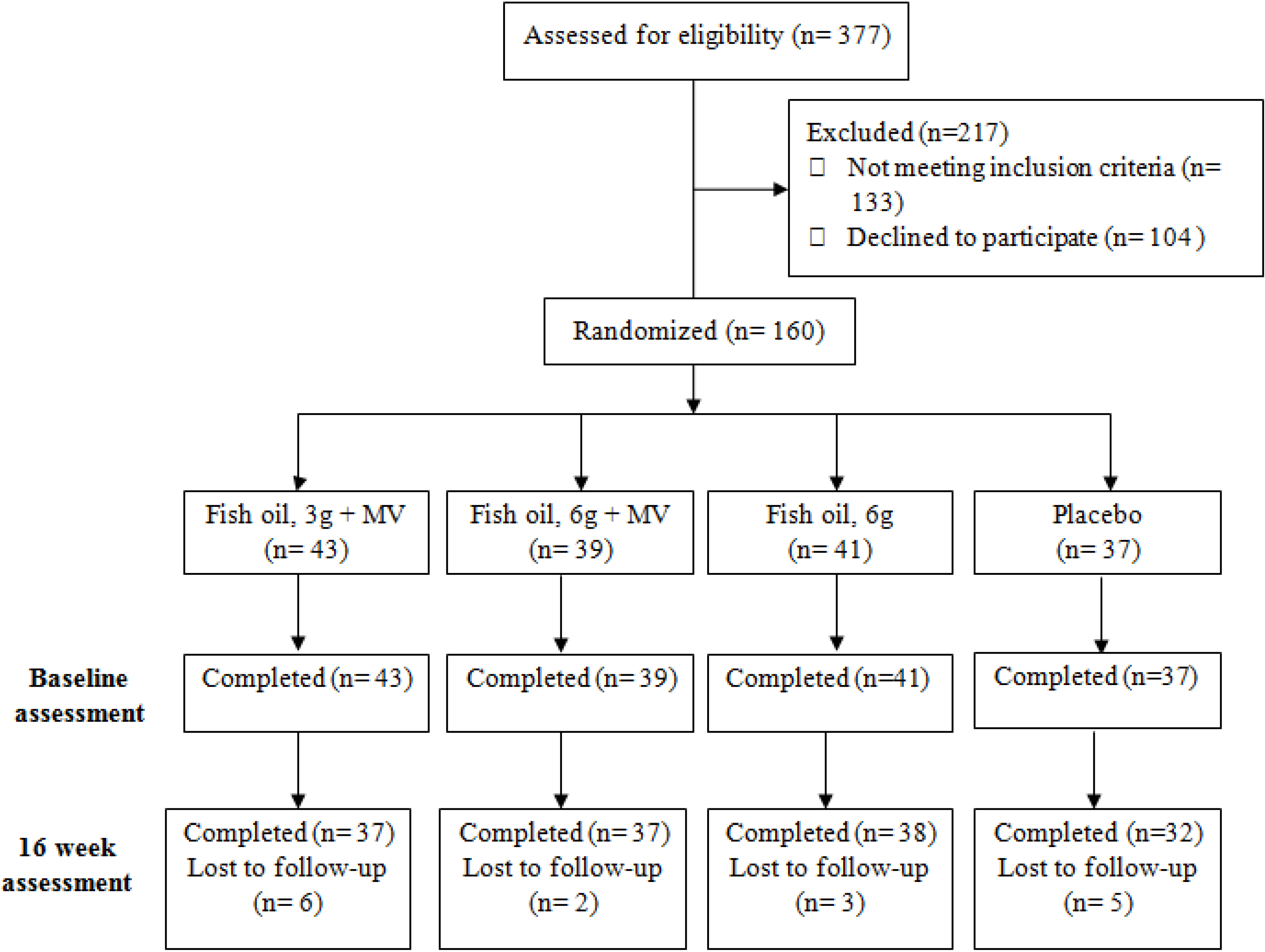
2.3. Interventions, Randomization and Blinding
- (1)
- Multivitamin combined with 3 g of fish oil (240 mg EPA and 240 mg DHA);
- (2)
- Multivitamin combined with 6 g of fish oil (480 mg EPA and 480 mg DHA);
- (3)
- Placebo multivitamin combined with 6 g fish oil (480 mg EPA and 480 mg DHA);
- (4)
- Placebo multivitamin combined with placebo fish oil (Sunola oil).
2.4. Outcomes Measures
2.5. Sample Size
2.6. Procedure
2.7. Statistical Analyses
3. Results
3.1. Cohort Demographics

{kind=link}
{kind=link}
{kind=link}
| Variable | Fish Oil, 3 g + Multivitamin | Fish Oil, 6 g + Multivitamin | Fish Oil, 6 g | Placebo | Overall |
|---|---|---|---|---|---|
| N | 43 | 39 | 41 | 37 | 160 |
| Age, year | 59.48 (5.64) | 58.90 (5.60) | 59.51 (5.89) | 59.19 (5.96) | 59.28 (5.72) |
| Male, % | 48 | 48 | 46 | 46 | 47 |
| Education, year | 15.54 (3.10) | 15.79 (3.92) | 15.84 (3.94) | 15.76 (3.38) | 15.73 (3.57) |
| MMSE | 28.12 (2.04) | 28.25 (1.61) | 28.07 (2.02) | 28.14 (1.74) | 28.14 (1.85) |
| Height, cm | 170.79 (8.79) | 169.63 (9.17) | 173.03 (9.91) | 170.23 (9.05) | 170.93 (9.24) |
| Weight, kg | 74.88 (13.78) | 70.98 (12.08) | 76.35 (16.28) | 70.35 (11.01) | 73.18 (13.57) |
| BMI | 25.54(3.59) | 24.41 (3.07) | 25.31 (4.03) | 24.2 (2.79) | 24.88 (3.43) |
| LDL, mmol/L | 3.31 (0.71) | 3.51 (0.72) | 3.37 (0.84) | 3.27 (0.72) | 3.36 (0.75) |
| HDL, mmol/L | 1.52 (0.42) | 1.61 (0.39) | 1.56 (0.44) | 1.57 (0.36) | 1.56 (0.40) |
| SBP, mmHg | 125.81 (20.97) | 122.59 (16.92) | 126.29 (16.92) | 121.41 (21.47) | 124.12 (19.10) |
| DBP, mmHg | 77.19 (13.32) | 75.46 (10.90) | 77.71 (9.82) | 74.62 (12.13) | 76.30 (11.58) |
3.2. Main Effects of Treatment on n-3 Fatty Acid and n-6 Fatty Acid Blood Measures
| Variable | Fish Oil, | Fish Oil, | Fish Oil, 6 g | Placebo | ANCOVA |
|---|---|---|---|---|---|
| 3 g + Multivitamin | 6 g + Multivitamin | F Value | |||
| EPA, % | 12.20 *** | ||||
| Baseline | 0.99 (0.46) | 1.01 (0.30) | 1.06 (0.41) | 1.00 (0.43) | |
| Week 16 | 1.41 (0.68) | 1.98 (0.65) *** | 1.66 (0.75) *** | 1.06 (0.48) | |
| % change | 42.42 | 96.04 | 56.60 | 6.00 | |
| DHA, % | 2.01 | ||||
| Baseline | 2.66 (1.26) | 2.74 (0.96) | 2.92 (1.10) | 2.82 (1.11) | |
| Week 16 | 2.94 (1.58) | 3.64 (1.27) | 3.16 (1.60) | 2.86 (1.21) | |
| % change | 10.53 | 32.85 | 8.22 | 1.42 | |
| DPA, % | 3.09 * | ||||
| Baseline | 1.69 (0.75) | 1.88 (0.50) | 1.94 (0.65) | 1.83 (0.61) | |
| Week 16 | 1.74 (0.85) | 2.31 (0.67) | 1.93 (0.96) | 1.87 (0.74) | |
| %change | 2.96 | 22.87 | −0.52 | 2.19 | |
| LC n-3 PUFA index, % | 3.98 ** | ||||
| Baseline | 5.34 (2.31) | 5.63 (1.59) | 5.92 (2.04) | 5.65 (2.00) | |
| Week 16 | 6.11 (2.99) | 7.92 (2.46) ** | 6.75 (3.23) | 5.79 (2.31) | |
| % change | 14.42 | 40.67 | 14.02 | 2.48 | |
| AA/EPA, ratio | 53.74 *** | ||||
| Baseline | 10.18 (4.06) | 10.18 (2.24) | 9.75 (3.20) | 10.58 (3.79) | |
| Week 16 | 6.11 (2.22) *** | 4.48 (1.05) *** | 4.64 (1.18) *** | 9.72 (3.13) | |
| % change | −39.98 | −55.99 | −52.41 | −8.13 | |
| Total n-3 FA, % | 3.96 * | ||||
| Baseline | 5.52 (2.32) | 5.83 (1.61) | 6.11 (2.06) | 5.85 (2.01) | |
| Week 16 | 6.26 (3.00) | 8.10 (2.47) ** | 6.90 (3.22) | 5.99 (2.32) | |
| % change | 13.41 | 38.94 | 12.93 | 2.39 | |
| Total n-6 FA, % | 4.01 ** | ||||
| Baseline | 21.97 (4.82) | 24.27 (3.42) | 23.80 (4.50) | 23.41 (4.49) | |
| Week 16 | 19.77 (5.60)* | 21.63 (4.34) | 19.98 (5.53) * | 23.66 (4.54) | |
| % change | −10.01 | −10.88 | −16.05 | 1.07 | |
| n-3/n-6 FA, ratio | 10.13 *** | ||||
| Baseline | 0.24 (0.78) | 0.23 (0.06) | 0.25 (0.07) | 0.24 (0.06) | |
| Week 16 | 0.29 (0.10) | 0.37 (0.09) *** | 0.33 (0.11) ** | 0.25 (0.08) | |
| % change | 20.83 | 60.86 | 32.00 | 4.17 | |
| n | 35 | 37 | 38 | 31 |
3.3. Effects of Treatment, Relative to Placebo, on n-3 Fatty Acid and n-6 Fatty Acid Blood Measures
3.4. Effects of Fish Oil Dosage on n-3 Fatty Acid and n-6 Fatty Acid Blood Measures
3.5. Effects of Combining Fish Oil with a Multivitamin on n-3 and n-6 Blood Measures
3.6. Sources of Variability in Red Blood Cell n-3 Fatty Acid Incorporation

3.7. Gender and Variability in n-3 Fatty Acid
| Variable | Fish Oil, | Fish Oil, | Fish Oil, | Placebo |
|---|---|---|---|---|
| 3g + Multivitamin | 6g + Multivitamin | 6 g | ||
| EPA | 0.48 | 0.33 | 0.45 | 0.45 |
| DHA | 0.54 | 0.35 | 0.51 | 0.42 |
| DPA | 0.49 | 0.29 | 0.50 | 0.40 |
| LC n-3 PUFA index | 0.49 | 0.31 | 0.48 | 0.40 |
| AA/EPA | 0.36 | 0.23 | 0.25 | 0.34 |
| Total n-3 | 0.48 | 0.30 | 0.47 | 0.39 |
| n-3/n-6 | 0.34 | 0.24 | 0.33 | 0.32 |

4. Discussion
5. Conclusions
Supplementary Files
Author Contributions
Conflicts of Interest
References
- Morgan, T.K.; Williamson, M.; Pirotta, M.; Stewart, K.; Myers, S.P.; Barnes, J. A national census of medicines use: A 24-h snapshot of Australians aged 50 years and older. Med. J. Aust. 2012, 196, 50–53. [Google Scholar]
- Rock, C.L. Multivitamin-multimineral supplements: Who uses them? Am. J. Clin. Nutr. 2007, 85, 277S–279S. [Google Scholar]
- Troesch, B.; Hoeft, B.; McBurney, M.; Eggersdorfer, M.; Weber, P. Dietary surveys indicate vitamin intakes below recommendations are common in representative Western countries. Br. J. Nutr. 2012, 108, 692–698. [Google Scholar] [CrossRef]
- Radimer, K.; Bindewald, B.; Hughes, J.; Ervin, B.; Swanson, C.; Picciano, M.F. Dietary supplement use by US adults: Data from the National Health and Nutrition Examination Survey, 1999–2000. Am. J. Epidemiol. 2004, 160, 339–349. [Google Scholar] [CrossRef]
- Stangl, G.I.; Kirchgessner, M. Different degrees of moderate iron deficiency modulate lipid metabolism of rats. Lipids 1998, 33, 889–895. [Google Scholar] [CrossRef]
- Bertrandt, J.; Klos, A.; Debski, B. Content of polyunsaturated fatty acids (PUFAs) in serum and liver of rats fed restricted diets supplemented with vitamins B2, B6 and folic acid. BioFactors 2004, 22, 189–192. [Google Scholar] [CrossRef]
- Durand, P.; Prost, M.; Blache, D. Pro-thrombotic effects of a folic acid deficient diet in rat platelets and macrophages related to elevated homocysteine and decreased n-3 polyunsaturated fatty acids. Atherosclerosis 1996, 121, 231–243. [Google Scholar] [CrossRef]
- Pase, M.P.; Grima, N.A.; Cockerell, R.; Stough, C.; Scholey, A.; Sali, A.; Pipingas, P. The effects of omega-3 fish oils and multivitamins on cognitive and cardiovascular function: A randomized, controlled clinical trial. J. Am. Coll. Nutr. 2014. [Google Scholar] [CrossRef]
- Harris, W.S.; Pottala, J.V.; Varvel, S.A.; Borowski, J.J.; Ward, J.N.; McConnell, J.P. Erythrocyte omega-3 fatty acids increase and linoleic acid decreases with age: Observations from 160,000 patients. Prostaglandins Leukot. Essent. Fat. Acids 2013, 88, 257–263. [Google Scholar] [CrossRef]
- Phang, M.; Lincz, L.F.; Garg, M.L. Eicosapentaenoic and docosahexaenoic acid supplementations reduce platelet aggregation and hemostatic markers differentially in men and women. J. Nutr. 2013, 143, 457–463. [Google Scholar] [CrossRef]
- Stonehouse, W.; Conlon, C.A.; Podd, J.; Hill, S.R.; Minihane, A.M.; Haskell, C.; Kennedy, D. DHA supplementation improved both memory and reaction time in healthy young adults: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 1134–1143. [Google Scholar] [CrossRef]
- Harris, W.S.; von Schacky, C. The omega-3 Index: A new risk factor for death from coronary heart disease? Prev. Med. 2004, 39, 212–220. [Google Scholar] [CrossRef]
- Stough, C.; Downey, L.; Silber, B.; Lloyd, J.; Kure, C.; Wesnes, K.; Camfield, D. The effects of 90-day supplementation with the omega-3 essential fatty acid docosahexaenoic acid (DHA) on cognitive function and visual acuity in a healthy aging population. Neurobiol. Aging 2012, 33, e1–e3. [Google Scholar] [CrossRef]
- Mazereeuw, G.; Lanctôt, K.L.; Chau, S.A.; Swardfager, W.; Herrmann, N. Effects of omega-3 fatty acids on cognitive performance: A meta-analysis. Neurobiol. Aging 2012, 33, e17–e29. [Google Scholar]
- Kalmijn, S.; van Boxtel, M.P.J.; Ocké, M.; Verschuren, W.M.; Kromhout, D.; Launer, L.J. Dietary intake of fatty acids and fish in relation to cognitive performance at middle age. Neurology 2004, 62, 275–280. [Google Scholar] [CrossRef]
- Nurk, E.; Drevon, C.A.; Refsum, H.; Solvoll, K.; Vollset, S.E.; Nygård, O.; Nygaard, H.A.; Engedal, K.; Tell, G.S.; Smith, A.D. Cognitive performance among the elderly and dietary fish intake: The Hordaland Health Study. Am. J. Clin. Nutr. 2007, 86, 1470–1478. [Google Scholar]
- Tully, A.M.; Roche, H.M.; Doyle, R.; Fallon, C.; Bruce, I.; Lawlor, B.; Coakley, D.; Gibney, M.J. Low serum cholesteryl ester-docosahexaenoic acid levels in Alzheimer’s disease: A case-control study. Br. J. Nutr. 2003, 89, 483–489. [Google Scholar] [CrossRef]
- Conquer, J.A.; Tierney, M.C.; Zecevic, J.; Bettger, W.J.; Fisher, R.H. Fatty acid analysis of blood plasma of patients with Alzheimer’s disease, other types of dementia, and cognitive impairment. Lipids 2000, 35, 1305–1312. [Google Scholar] [CrossRef]
- Huang, T.L. Omega-3 fatty acids, cognitive decline, and Alzheimer’s disease: A critical review and evaluation of the literature. J. Alzheimer Dis. 2010, 21, 673–690. [Google Scholar]
- Cao, J.; Schwichtenberg, K.A.; Hanson, N.Q.; Tsai, M.Y. Incorporation and clearance of omega-3 fatty acids in erythrocyte membranes and plasma phospholipids. Clin. Chem. 2006, 52, 2265–2272. [Google Scholar] [CrossRef]
- Katan, M.B.; Deslypere, J.P.; van Birgelen, A.P.; Penders, M.; Zegwaard, M. Kinetics of the incorporation of dietary fatty acids into serum cholesteryl esters, erythrocyte membranes, and adipose tissue: An 18-month controlled study. J. Lipid Res. 1997, 38, 2012–2022. [Google Scholar]
- Yurko-Mauro, K.; McCarthy, D.; Rom, D.; Nelson, E.B.; Ryan, A.S.; Blackwell, A.; Salem, N., Jr.; Stedman, M.; MIDAS Investigators. Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimer Dement. 2010, 6, 456–464. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pipingas, A.; Cockerell, R.; Grima, N.; Sinclair, A.; Stough, C.; Scholey, A.; Myers, S.; Croft, K.; Sali, A.; Pase, M.P. Randomized Controlled Trial Examining the Effects of Fish Oil and Multivitamin Supplementation on the Incorporation of n-3 and n-6 Fatty Acids into Red Blood Cells. Nutrients 2014, 6, 1956-1970. https://doi.org/10.3390/nu6051956
Pipingas A, Cockerell R, Grima N, Sinclair A, Stough C, Scholey A, Myers S, Croft K, Sali A, Pase MP. Randomized Controlled Trial Examining the Effects of Fish Oil and Multivitamin Supplementation on the Incorporation of n-3 and n-6 Fatty Acids into Red Blood Cells. Nutrients. 2014; 6(5):1956-1970. https://doi.org/10.3390/nu6051956
Chicago/Turabian StylePipingas, Andrew, Robyn Cockerell, Natalie Grima, Andrew Sinclair, Con Stough, Andrew Scholey, Stephen Myers, Kevin Croft, Avni Sali, and Matthew P. Pase. 2014. "Randomized Controlled Trial Examining the Effects of Fish Oil and Multivitamin Supplementation on the Incorporation of n-3 and n-6 Fatty Acids into Red Blood Cells" Nutrients 6, no. 5: 1956-1970. https://doi.org/10.3390/nu6051956