Improving the Metabolic and Mental Health of Children with Obesity: A School-Based Nutrition Education and Physical Activity Intervention in Wuhan, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
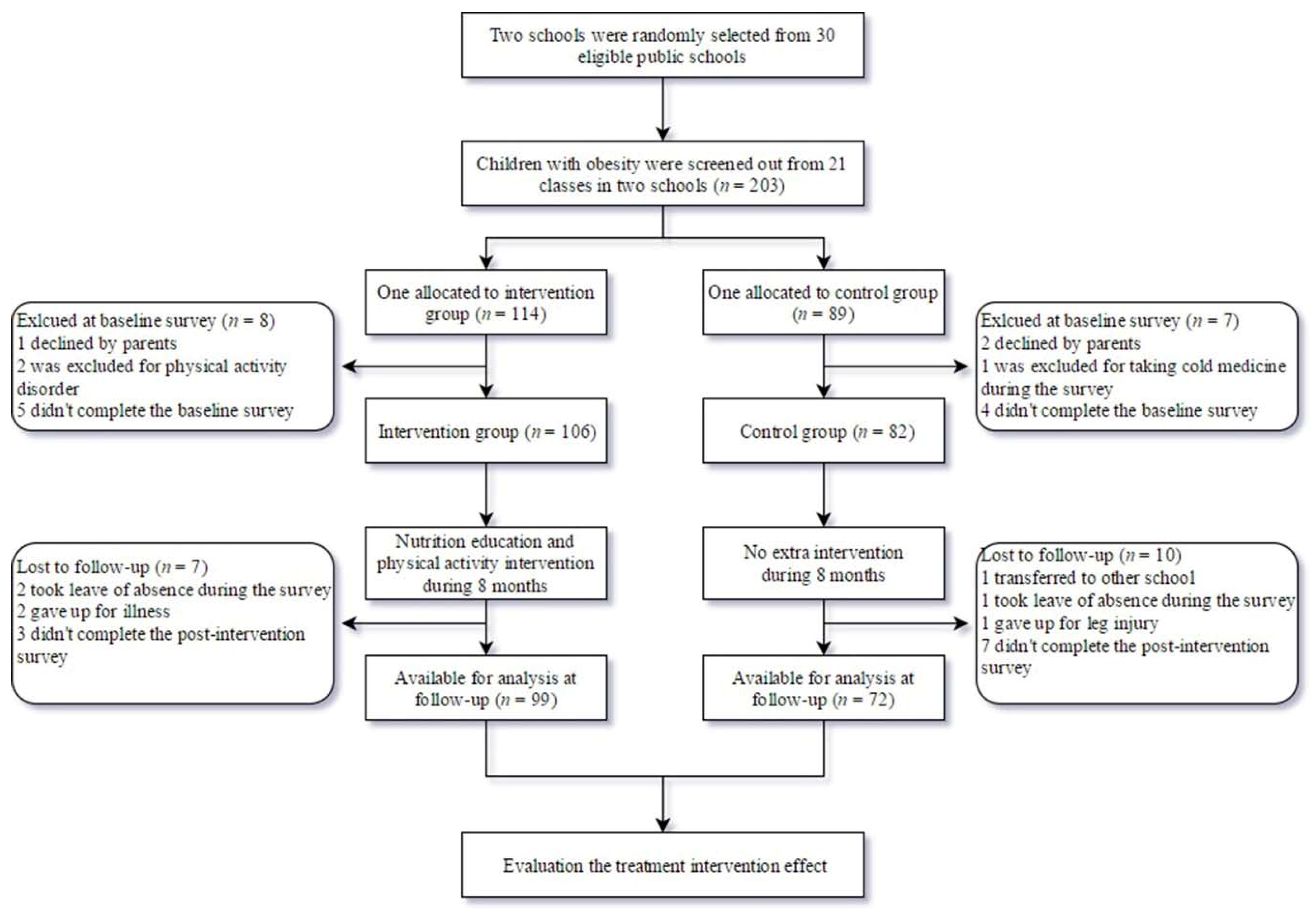
2.1. Study Design
2.2. Study Subjects
2.3. Intervention
2.4. Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the global burden of disease study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Zhou, Y.P.; Zhang, Q.; Wang, T.; Zhang, Y.Q.; Xu, B. Prevalence of overweight and obesity in chinese children and adolescents from 2015. Ann. Hum. Biol. 2017, 44, 642–643. [Google Scholar] [CrossRef]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A systematic review of australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Esposito, M.; Gallai, B.; Roccella, M.; Marotta, R.; Lavano, F.; Lavano, S.M.; Mazzotta, G.; Bove, D.; Sorrentino, M.; Precenzano, F.; et al. Anxiety and depression levels in prepubertal obese children: A case-control study. Neuropsychiatr. Dis. Treat. 2014, 10, 1897–1902. [Google Scholar]
- Wang, S.M.; Sun, Q.; Zhai, L.L.; Bai, Y.L.; Wei, W.; Jia, L.H. The prevalence of depression and anxiety symptoms among overweight/obese and non-overweight/non-obese children/adolescents in china: A systematic review and meta-analysis. Int. J. Environ. Res. Pub. Health 2019, 16, 340. [Google Scholar] [CrossRef] [Green Version]
- Llewellyn, A.; Simmonds, M.; Owen, C.G.; Woolacott, N. Childhood obesity as a predictor of morbidity in adulthood: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 56–67. [Google Scholar] [CrossRef]
- Ho, M.; Garnett, S.P.; Baur, L.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Effectiveness of lifestyle interventions in child obesity: Systematic review with meta-analysis. Pediatrics 2012, 130, E1647–E1671. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Wu, Y.; Cheskin, L.J.; Wilson, R.F.; Wang, Y. Effect of childhood obesity prevention programmes on blood lipids: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 933–944. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef]
- Hung, L.S.; Tidwell, D.K.; Hall, M.E.; Lee, M.L.; Briley, C.A.; Hunt, B.P. A meta-analysis of school-based obesity prevention programs demonstrates limited efficacy of decreasing childhood obesity. Nutr. Res. 2015, 35, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Wei, D.M.; Lin, S.T.; Maddison, R.; Ni Mhurchu, C.; Jiang, Y.; Gao, Y.; Wang, H.J. Systematic review and meta-analysis of school-based obesity interventions in mainland china. PLoS ONE 2017, 12, e0184704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Migueles, J.H.; Mora-Gonzalez, J.; Henriksson, P.; Martin-Matillas, M.; Mena-Molina, A.; Molina-Garcia, P.; Estevez-Lopez, F.; et al. Physical fitness and psychological health in overweight/obese children: A cross-sectional study from the activebrains project. J. Sci. Med. Sport 2018, 21, 179–184. [Google Scholar] [CrossRef]
- Yu, H.J.; Li, F.; Hu, Y.F.; Li, C.F.; Yang, X.H.; Yuan, S.; Huang, Y.; Tang, B.W.; Gong, J.; He, Q.Q. Associations of physical activity and fruit and vegetable intake with well-being and depressive symptoms among obese schoolchildren in wuhan, china: A cross-sectional study. BMC Public Health 2018, 18. [Google Scholar] [CrossRef]
- Ha, N.T.; Trang, D.T.H.; Ha, L.T.T. Is obesity associated with decreased health-related quality of life in school-age children?-results from a survey in vietnam. Aims Public Health 2018, 5, 338–351. [Google Scholar]
- Li, H.; Ji, C.Y.; Zong, X.N.; Zhang, Y.Q. Body mass index growth curves for chinese children and adolescents aged 0 to 18 years. Chin. J. Pediatr. 2009, 47, 493–498. [Google Scholar]
- Koo, H.C.; Poh, B.K.; Ruzita, A.T. Intervention on whole grain with healthy balanced diet to manage childhood obesity (great-childtrial): Study protocol for a quasi-experimental trial. SpringerPlus 2016, 5, 840. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.J.; Ma, L.; Ma, Y.H.; Wang, H.J.; Luo, J.Y.; Zhang, X.; Luo, C.Y.; Wang, H.; Zhao, H.P.; Pan, D.H.; et al. A national school-based health lifestyles interventions among chinese children and adolescents against obesity: Rationale, design and methodology of a randomized controlled trial in china. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [Green Version]
- Kaufman-Shriqui, V.; Fraser, D.; Friger, M.; Geva, D.; Bilenko, N.; Vardi, H.; Elhadad, N.; Mor, K.; Feine, Z.; Shahar, D.R. Effect of a school-based intervention on nutritional knowledge and habits of low-socioeconomic school children in israel: A cluster-randomized controlled trial. Nutrients 2016, 8, 234. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Li, Q.; Maddison, R.; Mhurchu, C.N.; Jiang, Y.N.; Wei, D.M.; Cheng, L.; Cheng, Y.; Wang, D.; Wang, H.J. A school-based comprehensive intervention for childhood obesity in china: A cluster randomized controlled trial. Child. Obes. 2019, 15, 105–115. [Google Scholar] [CrossRef]
- Li, F.F.; Wilkens, L.R.; Novotny, R.; Fialkowski, M.K.; Paulino, Y.C.; Nelson, R.; Bersamin, A.; Martin, U.; Deenik, J.; Boushey, C.J. Anthropometric measurement standardization in the us-affiliated pacific: Report from the children’s healthy living program. Am. J. Hum. Biol. 2016, 28, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Kuusikko, S.; Pollock-Wurman, R.; Ebeling, H.; Hurtig, T.; Joskitt, L.; Mattila, M.L.; Jussila, K.; Moilanen, I. Psychometric evaluation of social phobia and anxiety inventory for children (spai-c) and social anxiety scale for children-revised (sasc-r). Eur. Child Adoles. Psychiatry 2009, 18, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Su, L.Y.; Jin, Y. Norm of the screen for child social anxiety related emotional disorders in chinese urban children. Chin. J. Child Health Care 2006, 14, 335–337. [Google Scholar]
- Guo, H.T.; Zeng, X.S.; Zhuang, Q.Y.; Zheng, Y.B.; Chen, S.R. Intervention of childhood and adolescents obesity in shantou city. Obes. Res. Clin. Pract. 2015, 9, 357–364. [Google Scholar] [CrossRef]
- Lavelle, H.V.; Mackay, D.F.; Pell, J.P. Systematic review and meta-analysis of school-based interventions to reduce body mass index. J. Public Health 2012, 34, 360–369. [Google Scholar] [CrossRef] [Green Version]
- da Silveira, J.A.C.; Taddei, J.A.D.C.; Guerra, P.H.; Nobre, M.R.C. The effect of participation in school-based nutrition education interventions on body mass index: A meta-analysis of randomized controlled community trials. Prev. Med. 2013, 56, 237–243. [Google Scholar] [CrossRef]
- Mei, H.; Xiong, Y.L.; Xie, S.X.; Guo, S.Y.; Li, Y.K.; Guo, B.B.; Zhang, J.D. The impact of long-term school-based physical activity interventions on body mass index of primary school children - a meta-analysis of randomized controlled trials. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Almas, A.; Islam, M.; Jafar, T.H. School-based physical activity programme in preadolescent girls (9-11 years): A feasibility trial in karachi, pakistan. Arch. Dis. Child. 2013, 98, 515–519. [Google Scholar] [CrossRef]
- Seo, Y.G.; Lim, H.; Kim, Y.; Ju, Y.S.; Lee, H.J.; Jang, H.B.; Park, S.I.; Park, K.H. The effect of a multidisciplinary lifestyle intervention on obesity status, body composition, physical fitness, and cardiometabolic risk markers in children and adolescents with obesity. Nutrients 2019, 11, 137. [Google Scholar] [CrossRef] [Green Version]
- Miersch, A.; Vogel, M.; Gausche, R.; Siekmeyer, W.; Pfaffle, R.; Dittrich, K.; Kiess, W. Influence of seasonal variation on blood pressure measurements in children, adolescents and young adults. Pediatr. Nephrol. 2013, 28, 2343–2349. [Google Scholar] [CrossRef]
- Verduci, E.; Lassandro, C.; Giacchero, R.; Miniello, V.L.; Banderali, G.; Radaelli, G. Change in metabolic profile after 1-year nutritional-behavioral intervention in obese children. Nutrients 2015, 7, 10089–10099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, M.; Garnett, S.P.; Baur, L.A.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Impact of dietary and exercise interventions on weight change and metabolic outcomes in obese children and adolescents: A systematic review and meta-analysis of randomized trials. JAMA Pediatr. 2013, 167, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Shaodong, C.; Haihong, Z.; Manting, L.; Guohui, L.; Zhengxiao, Z.; Zhang, M.Z. Research of influence and mechanism of combining exercise with diet control on a model of lipid metabolism rat induced by high fat diet. Lipids Health Dis. 2013, 12, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, C.A.; Tyler, C.; Fullerton, G.; Poston, W.S.; Haddock, C.K.; McFarlin, B.; Reeves, R.S.; Foreyt, J.P. Results of an intensive school-based weight loss program with overweight mexican american children. Int. J. Pediatr. Obes. 2007, 2, 144–152. [Google Scholar] [CrossRef]
- Poeta, L.S.; Duarte Mde, F.; Caramelli, B.; Jorge, M.; Giuliano Ide, C. Effects of physical exercises and nutritional guidance on the cardiovascular risk profile of obese children. Revista da Associacao Medica Brasileira 2013, 59, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Morrison, K.M.; Shin, S.; Tarnopolsky, M.; Taylor, V.H. Association of depression & health related quality of life with body composition in children and youth with obesity. J. Affect. Disord. 2015, 172, 18–23. [Google Scholar]
- Lee, E.Y.; Spence, J.C. Pubertal development and screen time among south korean adolescents: Testing body mass index and psychological well-being as mediators. Glob. Health Res. Policy 2016, 1, 19. [Google Scholar] [CrossRef] [Green Version]
- Ruotsalainen, H.; Kyngas, H.; Tammelin, T.; Kaariainen, M. Systematic review of physical activity and exercise interventions on body mass indices, subsequent physical activity and psychological symptoms in overweight and obese adolescents. J. Adv. Nurs. 2015, 71, 2461–2477. [Google Scholar] [CrossRef]
- Hoare, E.; Fuller-Tyszkiewicz, M.; Skouteris, H.; Millar, L.; Nichols, M.; Allender, S. Systematic review of mental health and well-being outcomes following community-based obesity prevention interventions among adolescents. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [Green Version]
- Peyer, K.L.; Welk, G.; Bailey-Davis, L.; Yang, S.; Kim, J.K. Factors associated with parent concern for child weight and parenting behaviors. Child. Obes. 2015, 11, 269–274. [Google Scholar] [CrossRef]


{kind=link}
| Content | Targets | Concrete Techniques | Periods | Agent of Delivery |
|---|---|---|---|---|
| Supportive environment | Obtain teacher’s cooperation and supervision | (1) Understand the teaching plan for setting an appropriate exercise period to avoid interrupting the teaching plan and children’s academic achievements in the final exam. (2) Ensure the necessity of exercise facilities (rope and badminton, etc.). (3) Give instructions to let them know what, how and when to monitor the intervention on participants. | Initial stage | Designer and core members |
| Obtain parental participation and supervision | (1) Give a lecture for parents to learn the prevalence, cause, and harms of childhood obesity. (2) Deliver what needs to be supervised to parents, including limitation of screen time, preparation of a balanced diet, restricting intake of sugar-sweetened beverages, and ensuring adequate sleep and regular measurement of children’s body weight. (3) Encourage them to participate in health education lecture in class and physical activity at home with children. | Initial stage | Project members | |
| Advance health propaganda | (1) Chinese dietary guidelines including the food guide pyramid. (2) Physical activity guidelines. | Whole intervention | Project members | |
| Intervention implement | Compulsory exercise | (1) Jogging 20 min in the morning break every weekday. (2) Rope skipping 40 min on Monday and Thursday; play badminton 40 min on Wednesday and Friday; 200-m relay race 40 min on Tuesday. | Except the last month before final exam | Gym teachers |
| Lifestyle modification | (1) Health education class for children and parents in the class.Benefits of healthy lifestyles (physical activity and balanced diet); Harm of unhealthy lifestyles (sedentary behavior, western food, eating too fast, and skipping breakfast); How to persist in healthier habits and resist the temptation of unhealthy lifestyles. | Once every two months | Core members | |
| (2) Self-reported unhealthy lifestyles and setting goals to change them, sharing the goal with teachers and parents to supervise. | Teachers and parents | |||
| Quality control | Training | (1) Before the intervention, ensure all the project members experienced specialized training, including lecture skills, questionnaire survey method, and measurement of anthropometrics. (2) All the cardiovascular risk profiles were measured by professionals from the Centers for Disease Prevention and Control. | Initial stage | Designer and core members |
| Feedback | (1) Revise the intervention strategy according to the feedback from teachers and parents, especially the obstacles and success factors. | Once every two months | Core members | |
| Improve the education method | (1) Health education as much as possible in the form of animation to make it more attractive to children. (2) Use some games to review the health education context. (3) Adopt incentives to individuals who achieve the self-reported goals. | Whole intervention | Core members |
| Characteristics | Total (n = 171) | CG (n = 72) | IG (n = 99) | p Value a |
|---|---|---|---|---|
| Boys, n (%) | 136(79.5) | 54(75.0) | 82(82.8) | 0.251 |
| Age, years | 9.8(0.7) | 9.7(0.6) | 9.9(0.7) | 0.084 |
| Height, cm | 144.8(5.8) | 145.8(5.7) | 144.0(5.8) | 0.041 |
| Weight, kg | 51.2(7.2) | 51.9(6.7) | 50.6(7.5) | 0.119 |
| Monthly household income b, n (%) | ||||
| Low (<5000 Yuan RMB) | 71(43.8) | 27(42.2) | 44(44.9) | 0.383 |
| Middle (5000–10,000 Yuan RMB) | 67(41.4) | 30(46.9) | 37(37.8) | |
| High (>10,000 Yuan RMB) | 24(14.8) | 7(10.9) | 17(17.3) | |
| Outcomes | CG (n = 72) | p Value a | IG (n = 99) | p Value b | p Value c | p Value d | ||
|---|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | |||||
| Anthropometric indicators, mean (SD) | ||||||||
| BMI, kg/m2 | 24.3(1.9) | 24.5(2.4) | 0.346 | 24.3(2.5) | 24.4(2.7) | 0.348 | 0.585 | 0.675 |
| WC, cm | 82.4(5.7) | 85.1(5.8) | <0.001 | 81.5(6.6) | 84.0(10.1) | <0.001 | 0.651 | 0.468 |
| Cardiovascular risk profile, mean (SD) | ||||||||
| SBP, mmHg | 107.0(10.9) | 102.1(8.9) | 0.006 | 107.3(10.3) | 102.7(8.1) | <0.001 | 0.095 | 0.606 |
| DBP, mmHg | 71.3(7.0) | 68.5(6.5) | 0.002 | 74.6(8.0) | 67.4(6.1) | <0.001 | 0.017 | 0.275 |
| FPG, mmol/L | 4.6(0.5) | 5.1(0.4) | 0.002 | 5.0(0.4) | 4.6(0.5) | <0.001 | <0.001 | <0.001 |
| TG, mmol/L | 1.2(0.6) | 1.3(0.6) | 0.142 | 1.1(0.6) | 1.2(0.6) | 0.023 | 0.694 | 0.216 |
| HDL, mmol/L | 1.4(0.2) | 1.3(0.2) | 0.955 | 1.4(0.3) | 1.5(0.3) | 0.228 | 0.672 | 0.015 |
| Mental health, n (%) | ||||||||
| Poor well-being | 18(25.0) | 13(18.0) | 0.359 | 27(27.3) | 13(13.1) | 0.001 | 0.739 | 0.376 |
| Depression | 16(22.2) | 13(18.0) | 0.648 | 27(27.3) | 16(16.2) | 0.064 | 0.452 | 0.881 |
| Social anxiety | 16(22.2) | 20(27.8) | 0.388 | 30(30.3) | 20(20.2) | 0.137 | 0.239 | 0.321 |
| Outcomes | Time, Post | Group, Intervention | Group * Time | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β × 10 | 95% CI | pc | β × 10 | 95% CI | pc | β × 10 | 95% CI | pc | |
| Anthropometric indicators a | |||||||||
| BMI, kg/m2 | 0.08 | (−0.03, 0.18) | 0.152 | 0.05 | (−0.24, 0.35) | 0.720 | 0.01 | (−0.12, 0.14) | 0.886 |
| WC, cm | 0.30 | (0.17, 0.42) | <0.001 | 0.01 | (−0.23, 0.24) | 0.946 | −0.10 | (−0.39, 0.18) | 0.478 |
| Cardiovascular risk profile a | |||||||||
| SBP, mmHg | −0.41 | (−0.70, −0.12) | 0.005 | 0.47 | (0.17, 0.78) | <0.001 | −0.66 | (−1.03, −0.29) | <0.001 |
| DBP, mmHg | −0.42 | (−0.74, −0.11) | 0.008 | 0.12 | (−0.16, 0.41) | 0.401 | 0.01 | (−0.37, 0.38) | 0.972 |
| FPG, mmol/L | 0.02 | (0.00, 0.04) | 0.039 | 0.06 | (0.03, 0.09) | <0.001 | −1.24 | (−1.52, 1.43) | <0.001 |
| TG, mmol/L | 1.34 | (0.05, 2.62) | 0.042 | −0.07 | (−1.53, 1.38) | 0.922 | −0.02 | (−1.45, 1.40) | 0.975 |
| HDL, mmol/L | −0.49 | (−0.83, −0.15) | 0.005 | −0.18 | (−0.73, 0.38) | 0.533 | 0.87 | (0.48, 1.27) | <0.001 |
| Mental health b | |||||||||
| Poor well-being | −0.22 | (−0.97, 0.53) | 0.570 | 0.11 | (−0.64, 0.85) | 0.774 | −0.80 | (−1.7, 0.10) | 0.051 |
| Depression | −0.24 | (−1.05, 0.57) | 0.559 | 0.26 | (−0.48, 0.99) | 0.494 | −0.23 | (−1.21, 0.75) | 0.648 |
| Social anxiety | 0.52 | (−0.02, 1.07) | 0.059 | 0.37 | (−0.36, 1.10) | 0.324 | −0.75 | (−1.6, 0.09) | 0.029 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.-j.; Li, F.; Hu, Y.-f.; Li, C.-f.; Yuan, S.; Song, Y.; Zheng, M.; Gong, J.; He, Q.-q. Improving the Metabolic and Mental Health of Children with Obesity: A School-Based Nutrition Education and Physical Activity Intervention in Wuhan, China. Nutrients 2020, 12, 194. https://doi.org/10.3390/nu12010194
Yu H-j, Li F, Hu Y-f, Li C-f, Yuan S, Song Y, Zheng M, Gong J, He Q-q. Improving the Metabolic and Mental Health of Children with Obesity: A School-Based Nutrition Education and Physical Activity Intervention in Wuhan, China. Nutrients. 2020; 12(1):194. https://doi.org/10.3390/nu12010194
Chicago/Turabian StyleYu, Hong-jie, Fang Li, Yong-feng Hu, Chang-feng Li, Shuai Yuan, Yong Song, Miaobing Zheng, Jie Gong, and Qi-qiang He. 2020. "Improving the Metabolic and Mental Health of Children with Obesity: A School-Based Nutrition Education and Physical Activity Intervention in Wuhan, China" Nutrients 12, no. 1: 194. https://doi.org/10.3390/nu12010194