Dietary Intake and Sources of Potassium in a Cross-Sectional Study of Australian Adults

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Demographic and Anthropometric Data
2.3. Collection of 24 h Urine Data
2.4. Collection and Analysis of 24-h Dietary Recall Data
2.5. Comparison of Potassium Intakes to Dietary Guidelines
2.6. Categorising the Level of Processing of Foods Using NOVA Classification System
2.7. Classifying Foods into Core and Discretionary
2.8. Data Analysis
2.9. Ethical Approval
3. Results
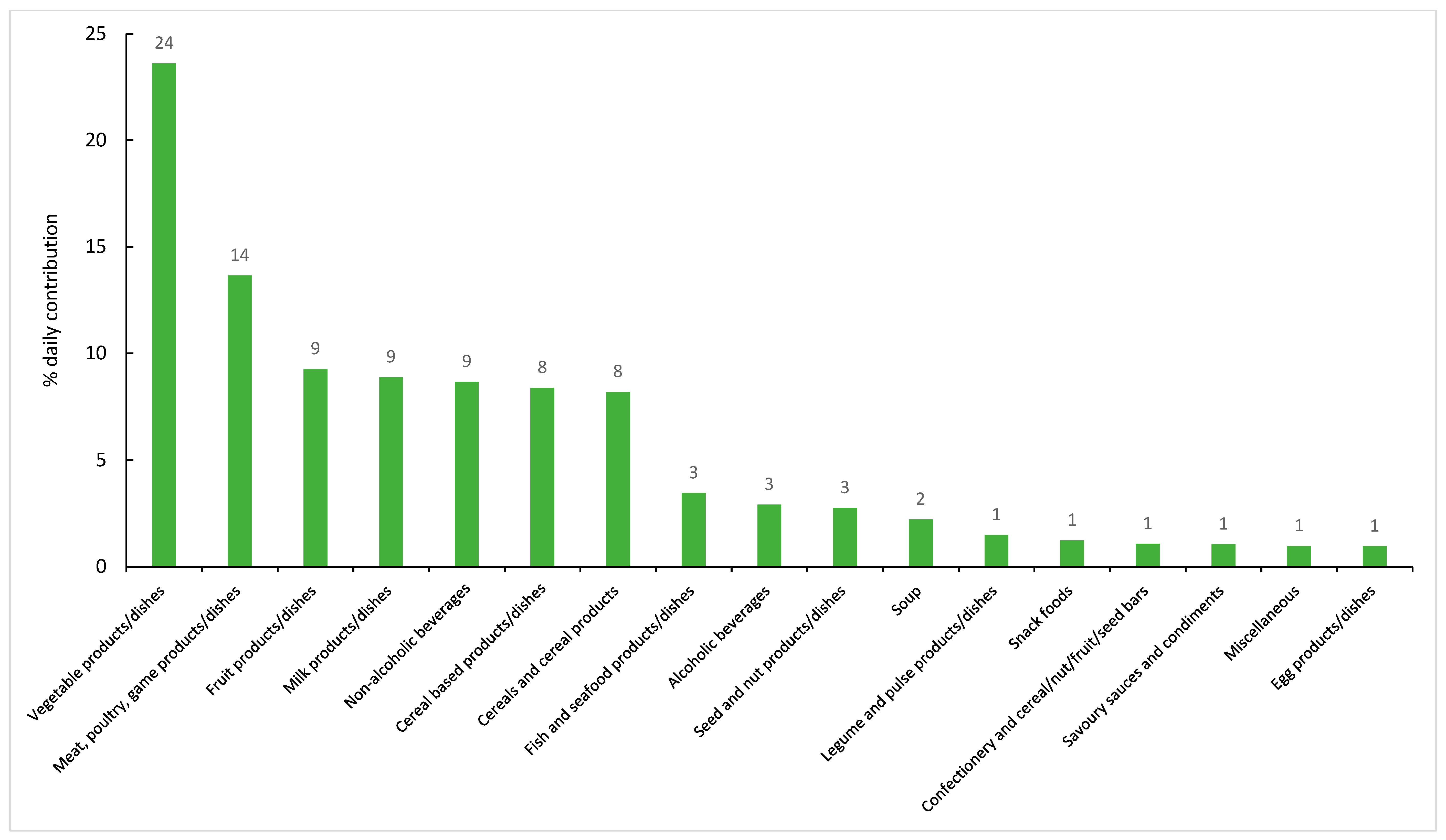
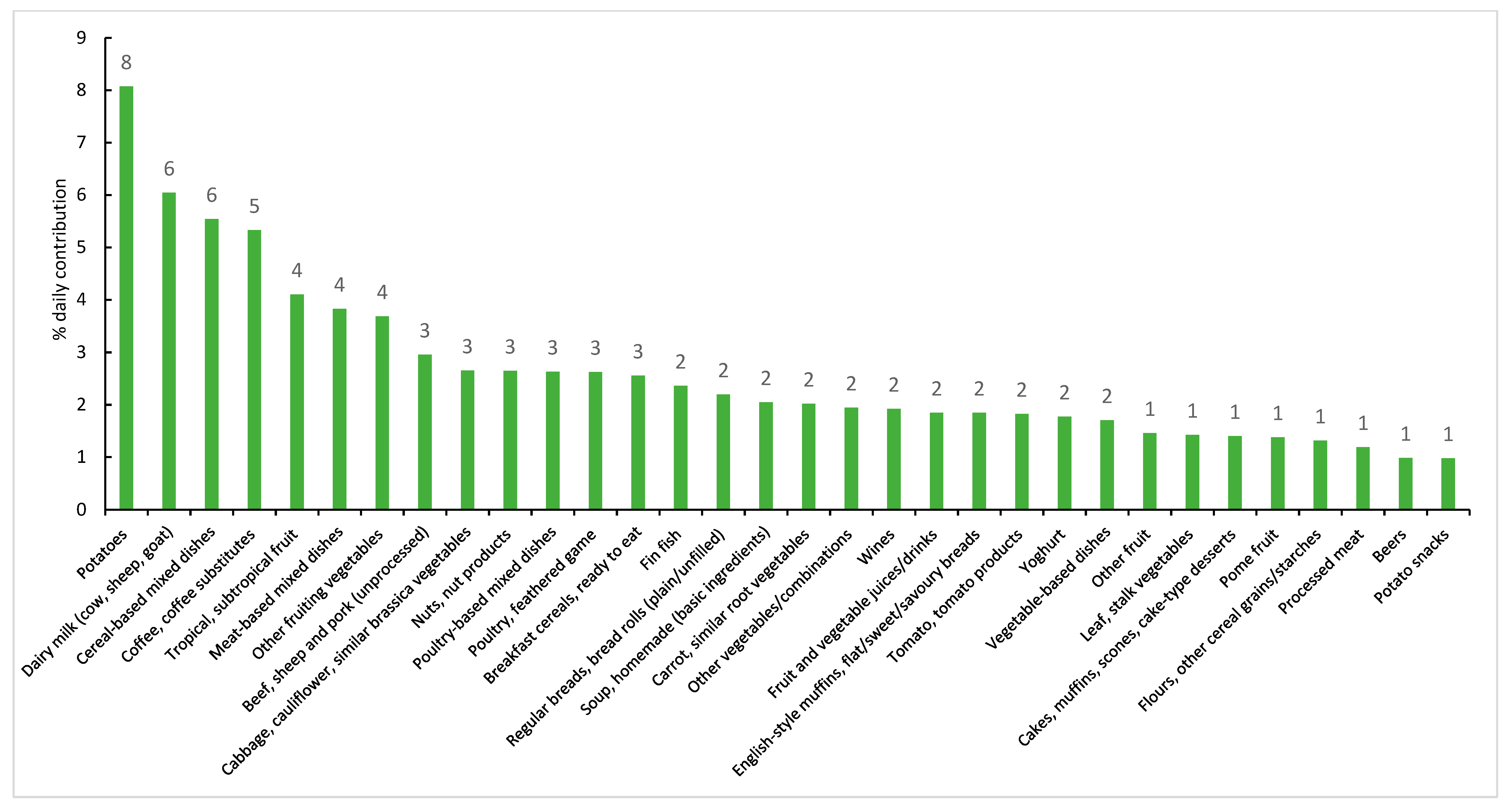
Food Sources of Potassium
4. Discussion
4.1. Potassium
4.2. Na:K
4.3. Sources of Dietary Potassium
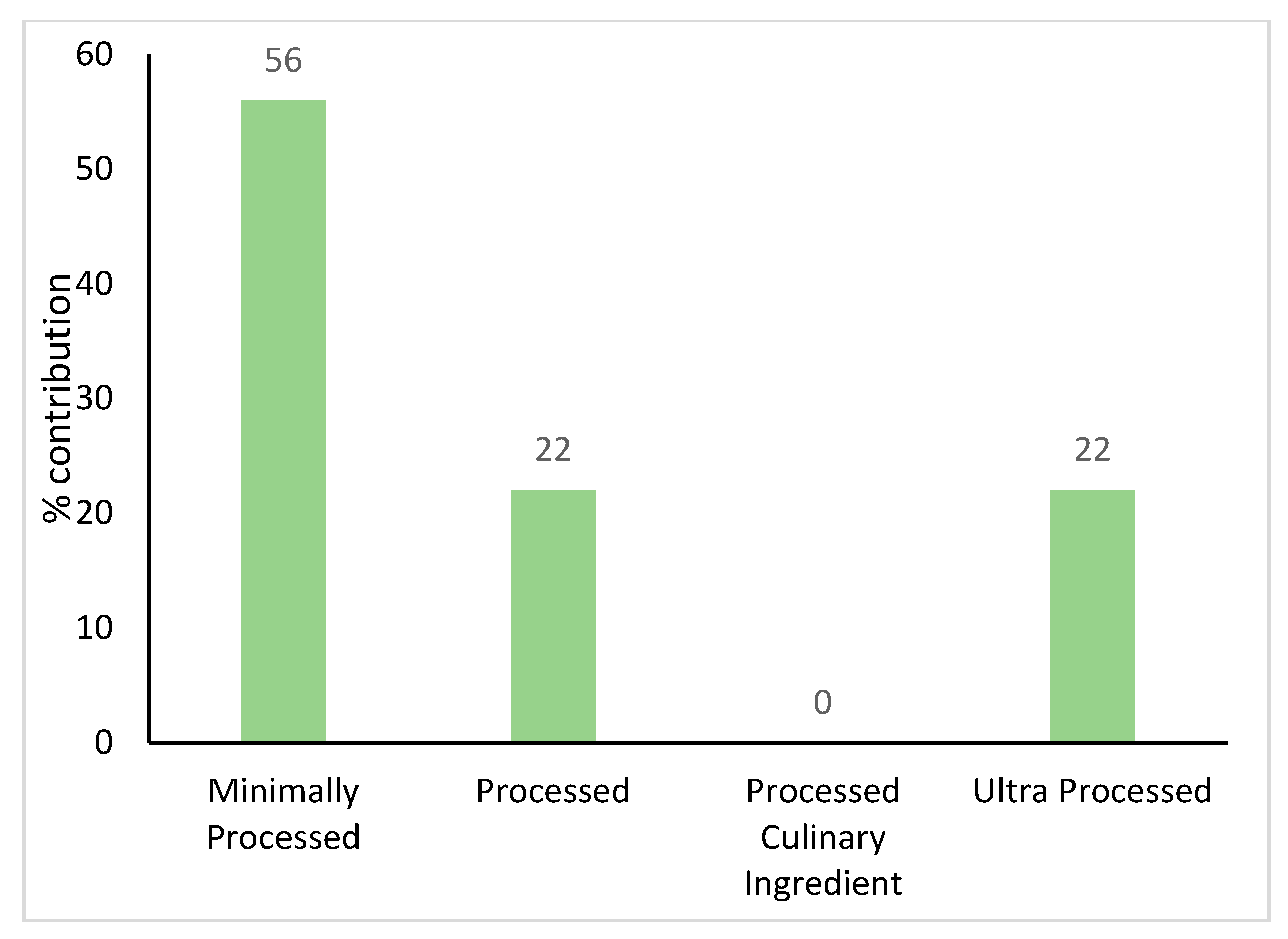
4.4. Level of Processing of Foods in Relation to Potassium Intake
4.5. Implications
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- 3303.0 Causes of Death, Australia. 2017. Available online: https://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/3303.0~2017~Main%20Features~Australia%27s%20leading%20causes%20of%20death,%202017~2 (accessed on 4 December 2019).
- Weaver, C.M. Potassium and health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Potassium. Available online: https://www.nrv.gov.au/nutrients/potassium (accessed on 30 September 2019).
- National Health and Medical Research Council. Summary. Recommendations to Reduce Chronic Disease Risk. Available online: https://www.nrv.gov.au/chronic-disease/summary (accessed on 11 September 2019).
- World Health Organization. Guideline: Potassium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010; USDA: Washington, DC, USA, 2011.
- Whelton, P.K.; He, J.; Cutler, J.A.; Brancati, F.L.; Appel, L.J.; Follmann, D.; Klag, M.J. Effects of oral potassium on blood pressure. Meta-analysis of randomized controlled clinical trials. JAMA 1997, 277, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, L.; Barba, G.; Cappuccio, F.P.; Strazzullo, P. Potassium intake, stroke, and cardiovascular disease a meta-analysis of prospective studies. J. Am. Coll. Cardiol. 2011, 57, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, J.; Trieu, K.; Dunford, E.; Nowson, C.; Jolly, K.A.; Greenland, R.; Reimers, J.; Bolam, B. Salt reduction in Australia: From advocacy to action. Cardiovasc. Diagn. Ther. 2015, 5, 207–218. [Google Scholar] [CrossRef]
- Trieu, K.; McMahon, E.; Santos, J.A.; Bauman, A.; Jolly, K.A.; Bolam, B.; Webster, J. Review of behaviour change interventions to reduce population salt intake. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 17. [Google Scholar] [CrossRef] [Green Version]
- VicHealth. State of Salt: The Case for Salt Reduction in Victoria. Available online: https://www.vichealth.vic.gov.au/media-and-resources/publications/state-of-salt (accessed on 4 September 2018).
- Iwahori, T.; Miura, K.; Ueshima, H. Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase. Nutrients 2017, 9, 700. [Google Scholar] [CrossRef]
- Adrogue, H.J.; Madias, N.E. The impact of sodium and potassium on hypertension risk. Semin. Nephrol. 2014, 34, 257–272. [Google Scholar] [CrossRef]
- Organization, W.H. Diet, Nutrition and the Prevention of Chronic Disease: Report of a Joint WHO/FAO Expert Consultation; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Trials of Hypertension Prevention Collaborative Research, G. Joint effects of sodium and potassium intake on subsequent cardiovascular disease: The Trials of Hypertension Prevention follow-up study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Beckford, K.; Baxter, J.R.; He, F.J.; Nowson, C.A. Dietary intake and sources of sodium and potassium among Australian schoolchildren: Results from the cross-sectional Salt and Other Nutrients in Children (SONIC) study. BMJ Open 2017, 7, e016639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowson, C.; Lim, K.; Grimes, C.; O’Halloran, S.; Land, M.A.; Webster, J.; Shaw, J.; Chalmers, J.; Smith, W.; Flood, V.; et al. Dietary Salt Intake and Discretionary Salt Use in Two General Population Samples in Australia: 2011 and 2014. Nutrients 2015, 7, 10501–10512. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 2016 Census QuickStats. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/2?opendocument (accessed on 1 May 2019).
- Department of Health. The Victorian Health Monitor; Department of Health and Human Services: Melbourne, Australia, 2012.
- World Health Organization. Body Mass Index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 16 August 2019).
- Australian Bureau of Statistics. 4363.0.55.001—Australian Health Survey: Users’ Guide, 2011-13. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4363.0.55.0012011-13?OpenDocument (accessed on 16 August 2019).
- Australian Bureau of Statistics. Australian Health Survey Food Model Booklet; ACT: Belconnen, Australia, 2010.
- Centres for Disease Control and Prevention. National Health and Nutrition Examination Survey MEC In-Person Dietary Interviewers Procedures Manual; Amazon: Seattle, WA, USA, 2017.
- Food Standards Australia New Zealand. AUSNUT 2011–2013. Available online: http://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/Pages/default.aspx (accessed on 16 August 2019).
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. S1), 5–41. [Google Scholar] [PubMed]
- Gibson, R. Principles of Nutritional Assessment; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Food Standards Agency. AUSNUT 2011–13 Food and Dietary Supplement Classification System. Available online: https://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/ausnutdatafiles/Pages/foodclassification.aspx (accessed on 25 November 2019).
- Moubarac, J.C.; Parra, D.C.; Cannon, G.; Monteiro, C.A. Food Classification Systems Based on Food Processing: Significance and Implications for Policies and Actions: A Systematic Literature Review and Assessment. Curr. Obes. Rep. 2014, 3, 256–272. [Google Scholar] [CrossRef]
- O’Halloran, S.A.; Grimes, C.A.; Lacy, K.E.; Campbell, K.J.; Nowson, C.A. Dietary Intake and Sources of Potassium and the Relationship to Dietary Sodium in a Sample of Australian Pre-School Children. Nutrients 2016, 8, 496. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. 4363.0.55.001—Australian Health Survey: Users’ Guide, 2011–13 Australian Health Survey—Discretionary Food List; Australian Bureau of Statistics: Adelaide, Australia, 2013.
- Australian Dietary Guidelines 2013. Available online: https://www.nutritionaustralia.org/national/resource/australian-dietary-guidelines-2013 (accessed on 4 December 2019).
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 23 December 2014).
- Krebs-Smith, S.M.; Kott, P.S.; Guenther, P.M. Mean proportion and population proportion: Two answers to the same question? J. Am. Diet. Assoc. 1989, 89, 671–676. [Google Scholar]
- Australian Bureau of Statistics. 3235.0 Regional Population by Age and Sex, Australia 2016. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/3235.0Main+Features12016?OpenDocument (accessed on 1 May 2019).
- Department of Health and Human Services. Victorian Population Health Survey 2016: Selected Survey Findings; Department of Health and Human Services: Melbourne, Australia, 2018.
- Miyagawa, N.; Okuda, N.; Nakagawa, H.; Takezaki, T.; Nishi, N.; Takashima, N.; Fujiyoshi, A.; Ohkubo, T.; Kadota, A.; Okamura, T.; et al. Socioeconomic Status Associated With Urinary Sodium and Potassium Excretion in Japan: NIPPON DATA2010. J. Epidemiol. 2018, 28 (Suppl. S3), S29–S34. [Google Scholar] [CrossRef] [Green Version]
- Elfassy, T.; Yi, S.S.; Llabre, M.M.; Schneiderman, N.; Gellman, M.; Florez, H.; Prado, G.; Zeki Al Hazzouri, A. Neighbourhood socioeconomic status and cross-sectional associations with obesity and urinary biomarkers of diet among New York City adults: The heart follow-up study. BMJ Open 2017, 7, e018566. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [Green Version]
- Loftfield, E.; Yi, S.; Curtis, C.J.; Bartley, K.; Kansagra, S.M. Potassium and fruit and vegetable intakes in relation to social determinants and access to produce in New York City. Am. J. Clin. Nutr. 2013, 98, 1282–1288. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, K.M.; Olstad, D.L.; Leech, R.M.; Ball, K.; Meertens, B.; Potter, J.; Cleanthous, X.; Reynolds, R.; McNaughton, S.A. Socioeconomic Inequities in Diet Quality and Nutrient Intakes among Australian Adults: Findings from a Nationally Representative Cross-Sectional Study. Nutrients 2017, 9, 1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athanasatou, A.; Kandyliari, A.; Malisova, O.; Pepa, A.; Kapsokefalou, M. Sodium and Potassium Intake from Food Diaries and 24-h Urine Collections from 7 Days in a Sample of Healthy Greek Adults. Front. Nutr. 2018, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Afzalpurkar, R.; Fordtran, J.S. Pathophysiology of potassium absorption and secretion by the human intestine. Gastroenterology 1994, 107, 548–571. [Google Scholar] [CrossRef]
- Tasevska, N.; Runswick, S.A.; Bingham, S.A. Urinary potassium is as reliable as urinary nitrogen for use as a recovery biomarker in dietary studies of free living individuals. J. Nutr. 2006, 136, 1334–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holbrook, J.T.; Patterson, K.Y.; Bodner, J.E.; Douglas, L.W.; Veillon, C.; Kelsay, J.L.; Mertz, W.; Smith, J.C., Jr. Sodium and potassium intake and balance in adults consuming self-selected diets. Am. J. Clin. Nutr. 1984, 40, 786–793. [Google Scholar] [CrossRef]
- Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Available online: https://www.nal.usda.gov/sites/default/files/fnic_uploads/energy_full_report.pdf (accessed on 4 December 2019).
- Dickinson, K.M.; Chan, L.; Moores, C.J.; Miller, J.; Thomas, J.; Yaxley, A.; Jackson, K.; Mehta, K.; Matwiejczyk, L.; Wray, A.; et al. Eating occasions and the contribution of foods to sodium and potassium intakes in adults. Public Health Nutr. 2018, 21, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Parker, E.A.; Rhodes, D.G.; Goldman, J.D.; Clemens, J.C.; Moshfegh, A.J.; Thuppal, S.V.; Weaver, C.M. Estimating Sodium and Potassium Intakes and Their Ratio in the American Diet: Data from the 2011-2012 NHANES. J. Nutr. 2016. [Google Scholar] [CrossRef]
- Cogswell, M.E.; Loria, C.M.; Terry, A.L.; Zhao, L.; Wang, C.Y.; Chen, T.C.; Wright, J.D.; Pfeiffer, C.M.; Merritt, R.; Moy, C.S.; et al. Estimated 24-Hour Urinary Sodium and Potassium Excretion in US Adults. JAMA 2018, 319, 1209–1220. [Google Scholar] [CrossRef]
- Derbyshire, E. Micronutrient Intakes of British Adults Across Mid-Life: A Secondary Analysis of the UK National Diet and Nutrition Survey. Front. Nutr. 2018, 5, 55. [Google Scholar] [CrossRef] [Green Version]
- Meneton, P.; Lafay, L.; Tard, A.; Dufour, A.; Ireland, J.; Menard, J.; Volatier, J.L. Dietary sources and correlates of sodium and potassium intakes in the French general population. Eur. J. Clin. Nutr. 2009, 63, 1169–1175. [Google Scholar] [CrossRef] [Green Version]
- Margerison, C.; Riddell, L.J.; Wattanapenpaiboon, N.; Nowson, C. Dietary sources and meal distribution of sodium and potassium in a sample of Australian adults. Nutr. Diet. 2013, 70, 294–299. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 4364.0.55.007—Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011–12; Australian Bureau of Statistics, Ed.; Commonwealth of Australia: Canberra, Australia, 2014.
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14 (Suppl. S2), 21–28. [Google Scholar] [CrossRef] [PubMed]
- Slimani, N.; Deharveng, G.; Southgate, D.A.; Biessy, C.; Chajes, V.; van Bakel, M.M.; Boutron-Ruault, M.C.; McTaggart, A.; Grioni, S.; Verkaik-Kloosterman, J.; et al. Contribution of highly industrially processed foods to the nutrient intakes and patterns of middle-aged populations in the European Prospective Investigation into Cancer and Nutrition study. Eur. J. Clin. Nutr. 2009, 63 (Suppl. S4), S206–S225. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baraldi, L.G.; Martinez Steele, E.; Canella, D.S.; Monteiro, C.A. Consumption of ultra-processed foods and associated sociodemographic factors in the USA between 2007 and 2012: Evidence from a nationally representative cross-sectional study. BMJ Open 2018, 8, e020574. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Moubarac, J.C.; Levy, R.B.; Canella, D.S.; Louzada, M.; Cannon, G. Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.; White, M. Characterisation of UK diets according to degree of food processing and associations with socio-demographics and obesity: Cross-sectional analysis of UK National Diet and Nutrition Survey (2008–12). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 160. [Google Scholar] [CrossRef] [Green Version]
- Juul, F.; Hemmingsson, E. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public Health Nutr. 2015, 18, 3096–3107. [Google Scholar] [CrossRef] [Green Version]
- Martinez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients 2012, 4, 2097–2120. [Google Scholar] [CrossRef] [Green Version]
- Dwyer, J.T.; Fulgoni, V.L., III; Clemens, R.A.; Schmidt, D.B.; Freedman, M.R. Is “ processed” a four-letter word? The role of processed foods in achieving dietary guidelines and nutrient recommendations. Adv. Nutr. 2012, 3, 536–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moubarac, J.C.; Batal, M.; Martins, A.P.; Claro, R.; Levy, R.B.; Cannon, G.; Monteiro, C. Processed and ultra-processed food products: Consumption trends in Canada from 1938 to 2011. Can. J. Diet. Pract. Res. 2014, 75, 15–21. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.M.; Farmer, V.L.; Nettleton, A.; Cameron, C.M.; Cook, N.R.; Woodward, M.; Campbell, N.R.C.; Consortium, T. Twenty-Four-Hour Diet recall and Diet records compared with 24-hour urinary excretion to predict an individual’s sodium consumption: A Systematic Review. J. Clin. Hypertens. (Greenwich) 2018, 20, 1360–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Rehm, C.D. Sodium intakes of US children and adults from foods and beverages by location of origin and by specific food source. Nutrients 2013, 5, 1840–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Proportion (%) or Median | ||||
|---|---|---|---|---|
| Total n = 338 | Males n = 148 (49%) | Females n = 190 (51%) | Victorian Population (%)49% Males, 51% Females a | |
| Age (years) * | 41.2 (13.9) | 41.0 (13.4) | 41.4 (14.3) | 37 a |
| Age group (years) | ||||
| 18–34 | 38 | 39 | 38 | 29 b |
| 35–54 | 42 | 42 | 42 | 26 |
| 55–65 | 20 | 20 | 20 | 11 |
| BMI * | 24.6 (4.1) | 25.3 (3.5) | 24.0 (4.5) | |
| BMI category | ||||
| Underweight | 3 | 2 | 5 | 2 c |
| Healthy weight | 53 | 47 | 59 | 38 |
| Overweight | 35 | 42 | 28 | 31 |
| Obese | 9 | 10 | 9 | 19 |
| Socioeconomic disadvantage (quintiles) | ||||
| 1st quintile (greatest disadvantage) | 6.3 | 2.9 | 9.5 | |
| 2nd quintile | 6.7 | 7.0 | 6.4 | |
| 3rd quintile | 9.2 | 9.5 | 8.8 | |
| 4th quintile | 34.8 | 39.8 | 29.9 | |
| 5th quintile (least disadvantage) | 43.1 | 40.8 | 45.3 | |
| Measure | Total | Age Group (Years) | p Value | Males | Females | p Value | Socioeconomic Disadvantage (Quintiles) | p Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Urinary Data | n = 338 | 18–34 n = 63 | 35–54 n = 155 | 55–65 n = 120 | Total n = 148 | Total n = 190 | 1 n = 23 | 2 n = 21 | 3 n = 40 | 4 n = 104 | 5 n = 150 | |||
| Urinary K (mmol/24-h) Mean (95%CI) | 76.8 (73.0–80.5) | 74.4 (66.5–82.3) | 78.6 (73.7–83.4) | 77.7 (73.1–82.2) | 0.67 | 88.4 (82.3–94.4) | 65.5 (62.6–68.6) | <0.001 | 61.0 b (54.1–68.0) | 80.5 (67.0–94.0) | 74.6 (64.9–84.3) | 77.5 (70.6–84.3) | 78.4 (72.7–84.0) | <0.002 |
| Urinary K (mmol/24-h) Median (IQR) | 71.5 (55.9–91.3) | 68.1 (55.6–89.0) | 73.7 (58.2–94.6) | 73.9 (60.0–89.0) | 86.4 (64.8–105.4) | 64.5 (49.2–79.9) | 55.6 (49.5–73.6) | 77.9 (59.6–96.9) | 65.0 (58.6–85.2) | 77.0 (57.2–90.1) | 73.3 (58.3–100.9) | |||
| Urinary Na:K (mmol/24-h) Mean (95%CI) | 1.9 (1.8–2.0) | 2.0 a (1.8–2.3) | 1.8 (1.7–2.0) | 1.7 (1.6–1.9) | 0.09 | 2.0 (1.8–2.1) | 1.8 (1.7–1.9) | 0.16 | 2.3 (1.8–2.8) | 1.8 (1.5–2.1) | 2.0 (1.7–2.3) | 2.0 (1.8–2.2) | 1.8 (1.6–1.9) | 0.13 |
| Diet Recall Data | Total n = 142 | 18–34 n = 28 | 35–54 n = 79 | 55–65 n = 35 | p value | Total n = 148 | Total n = 190 | p value | 1 n = 11 | 2 n = 7 | 3 n = 21 | 4 n = 31 | 5 n = 72 | p value |
| K diet recall (mmol/24-h) Mean (95%CI) | 92.9 (86.6–99.1) | 85.4 (73.7–97.2) | 95.2 (88.3–102.1) | 102.6 (89.7–115.6) | 0.14 | 100.2 (88.5–111.8) | 85.8 (79.4–92.3) | <0.04 | 97.1 (71.1–123.2) | 76.0 (52.5–99.5) | 96.4 (85.7–107.0) | 95.1 (83.2–107.0) | 91.9 (82.7–101.0) | 0.62 |
| K diet recall (mmol/24-h) Median (IQR) | 85.1 (70.5–111.0) | 80.0 (70.5–103.6) | 86.0 (71.0–118.5) | 103.2 (68.9–126.7) | 102.9 (70.5–120.9) | 81.2 (68.3–101.8) | 86.0 (69.9–104.9) | 63.5 (59.2–80.3) | 94.1 (81.3–109.4) | 86.8 (80.0–108.8) | 82.5 (70.5–114.5) | |||
| NA:K diet (mmol/24-h) Mean (95%CI) | 1.4 (1.2–1.7) | 1.6 (1.1–2.2) | 1.3 (1.2–1.5) | 1.1 (0.9–1.3) | 0.12 | 1.5 (1.0–2.0) | 1.3 (1.2–1.5) | 0.45 | 1.3 (1.0–1.5) | 1.7 (1.2–2.3) | 1.4 (1.1–1.7) | 1.3 (0.9–1.6) | 1.5 (1.1–1.9) | 0.61 |
| Energy (kJ/day) diet recall Mean (95%CI) | 10,043.2 (9457.4–10,629.1) | 9973.6 (8662.8–11,284.4) | 10,223.9 (9653.0–10,794.7) | 9791.2 (8876.1–10,706.4) | 0.72 | 10,827.6 (9817.1–11,838.1) | 9284.9 (8708.0–9861.8) | <0.01 | 9712.1 (8328–11,095.9) | 10,327.6 (7920.4–12,734.8) | 10,478.8 (9711.7–11,245.9) | 10,136.1 (8257.4–12,014.7) | 9919.5 (9343.7–10,495.3) | 0.80 |
| Potassium density (g potassium/MJ energy) | 0.37 (0.35–0.39) | 0.35 (0.30–0.40) | 0.37 (0.35–0.39) | 0.41 (0.37–0.45) | 0.07 | 0.37 (0.33–0.41) | 0.37 (0.35–0.40) | 0.88 | 0.38 (0.32–0.44) | 0.30 (0.23–0.37) | 0.36 (0.32–0.40) | 0.39 (0.34–0.44) | 0.37 (0.33–0.41) | 0.41 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolton, K.A.; Trieu, K.; Woodward, M.; Nowson, C.; Webster, J.; Dunford, E.K.; Bolam, B.; Grimes, C. Dietary Intake and Sources of Potassium in a Cross-Sectional Study of Australian Adults. Nutrients 2019, 11, 2996. https://doi.org/10.3390/nu11122996
Bolton KA, Trieu K, Woodward M, Nowson C, Webster J, Dunford EK, Bolam B, Grimes C. Dietary Intake and Sources of Potassium in a Cross-Sectional Study of Australian Adults. Nutrients. 2019; 11(12):2996. https://doi.org/10.3390/nu11122996
Chicago/Turabian StyleBolton, Kristy A., Kathy Trieu, Mark Woodward, Caryl Nowson, Jacqui Webster, Elizabeth K. Dunford, Bruce Bolam, and Carley Grimes. 2019. "Dietary Intake and Sources of Potassium in a Cross-Sectional Study of Australian Adults" Nutrients 11, no. 12: 2996. https://doi.org/10.3390/nu11122996