Salt Preference and Ability to Discriminate between Salt Content of Two Commercially Available Products of Australian Primary Schoolchildren


Abstract
:1. Introduction
2. Methods
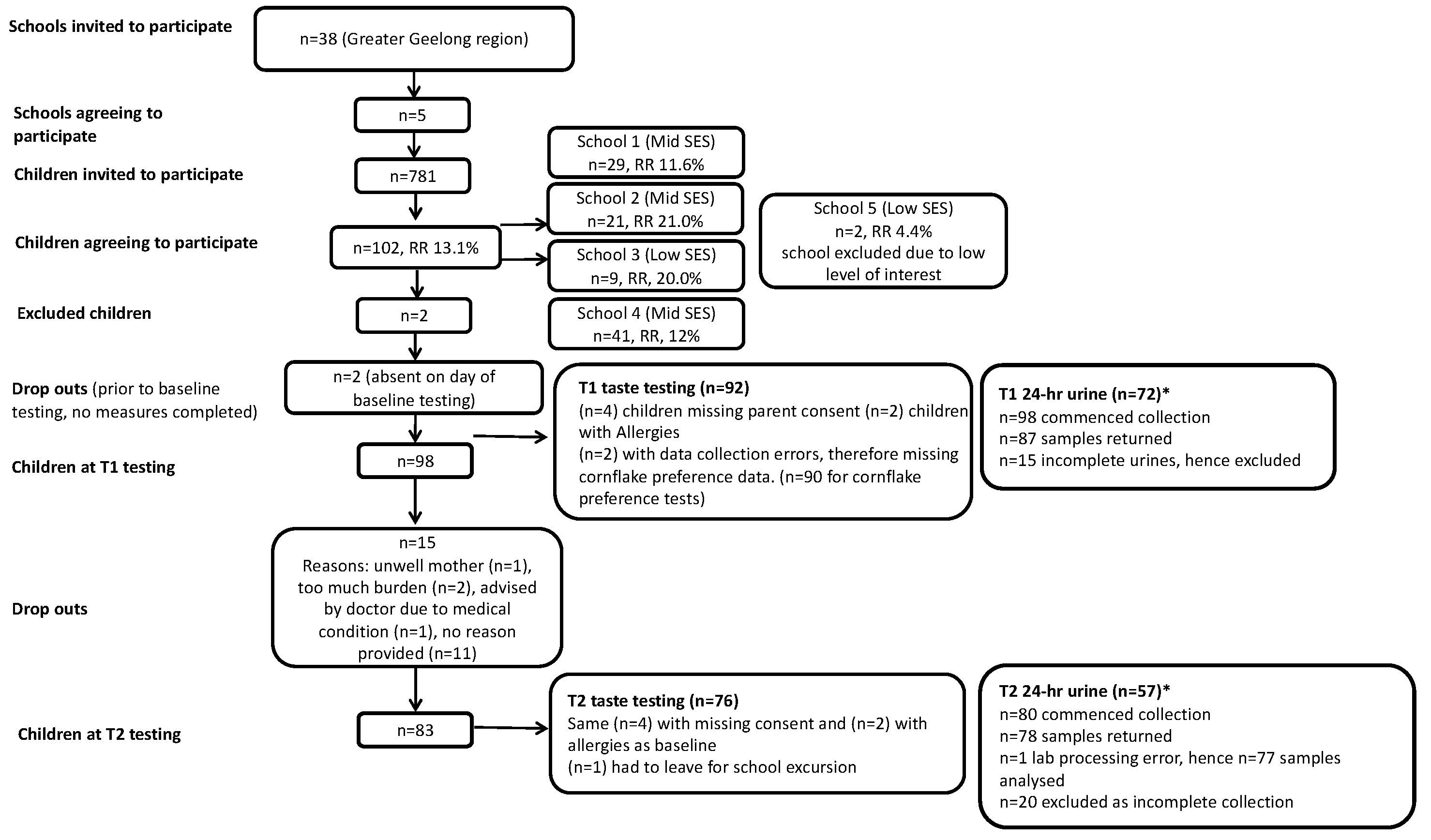
2.1. Study Design and Participants
2.2. Data Collection
2.3. Demographic Characteristics
2.4. 24-h Urine Collection
2.5. Anthropometry
2.6. Taste Testing
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Salt Preference
3.3. Ability to Rank Samples (ARS) According to Salt Content
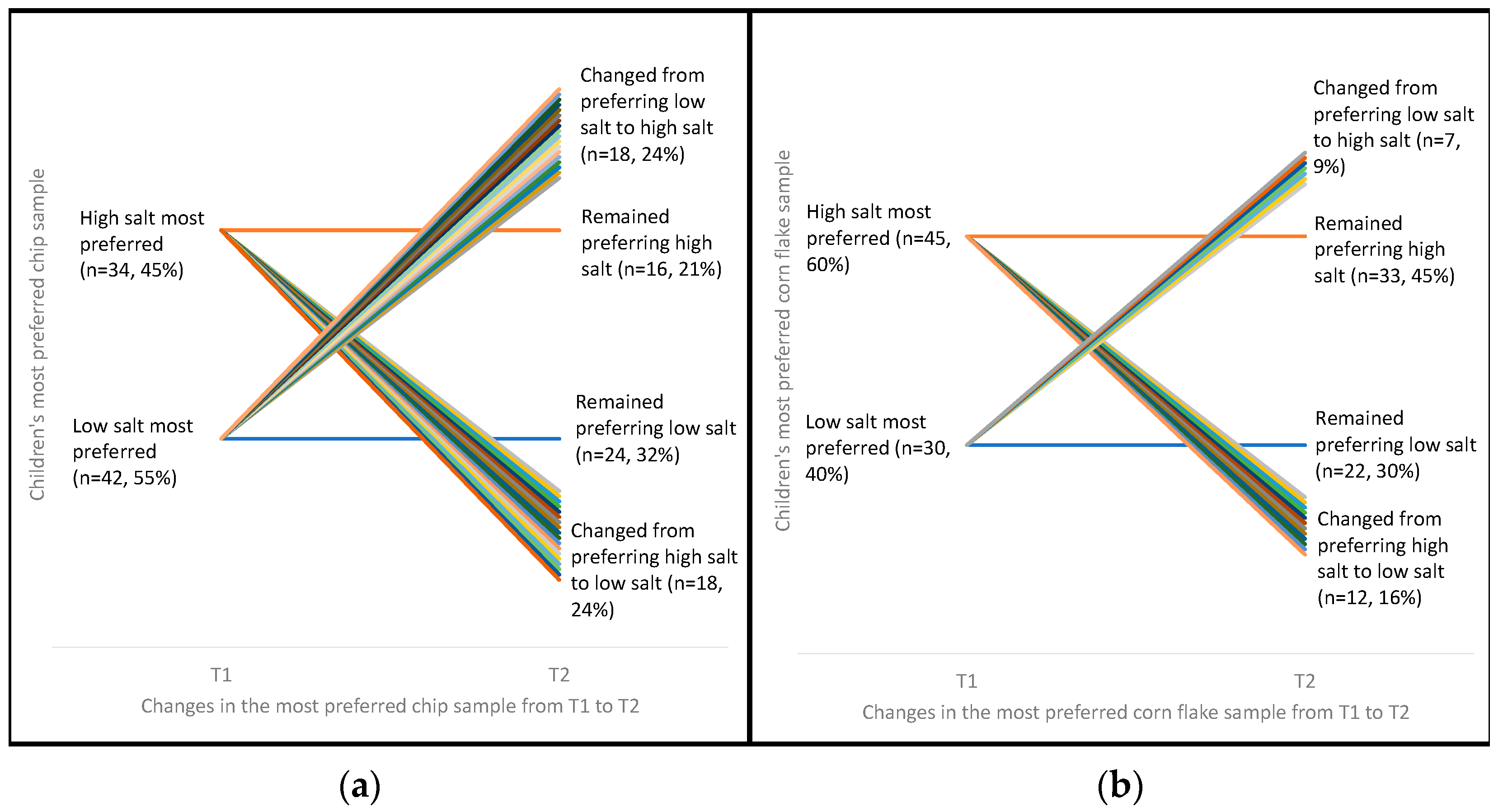
3.4. Changes in Salt Preference from Time Point (T1) to Time Point 2 (T2)
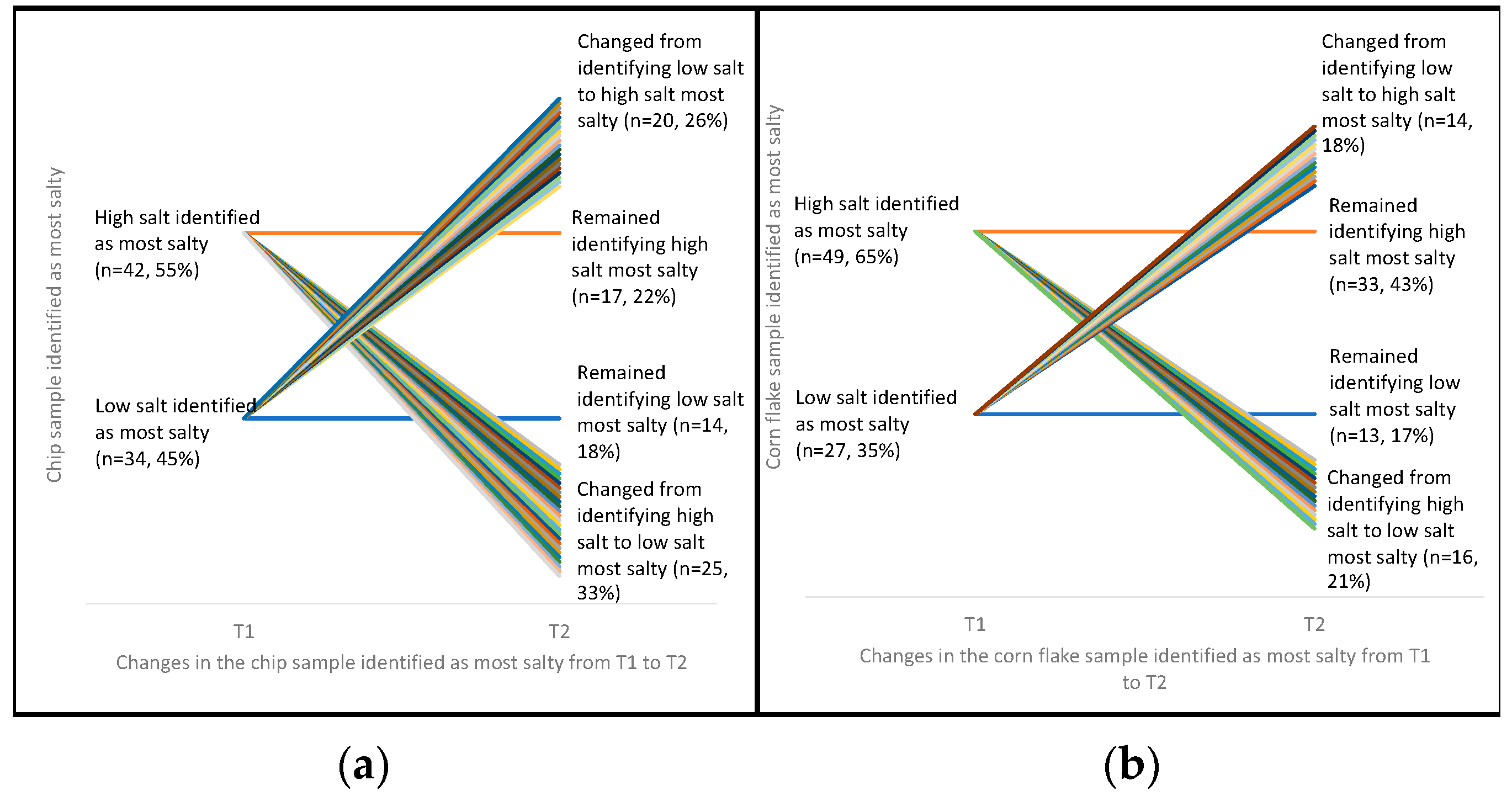
3.5. Changes in Ability to Rank Samples (ARS) according to Salt Content from T1 to T2
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beauchamp, G.K.; Cowart, B.J. Preference for high salt concentrations among children. Dev. Psychol. 1990, 26, 539–545. [Google Scholar] [CrossRef]
- Mennella, J.A.; Finkbeiner, S.; Lipchock, S.V.; Hwang, L.D.; Reed, D.R. Preferences for salty and sweet tastes are elevated and related to each other during childhood. PLoS ONE 2014, 9, e92201. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Beckford, K.; Baxter, J.R.; He, F.J.; Nowson, C.A. Dietary intake and sources of sodium and potassium among Australian schoolchildren: Results from the cross-sectional Salt and Other Nutrients in Children (SONIC) study. BMJ Open 2017, 7, e016639. [Google Scholar] [CrossRef] [PubMed]
- Land, M.A.; Neal, B.C.; Johnson, C.; Nowson, C.A.; Margerison, C.; Petersen, K.S. Salt consumption by Australian adults: A systematic review and meta-analysis. Med. J. Aust. 2018, 208, 75–81. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Mennella, J.A.; Spector, A.C.; Reed, D.R.; Coldwell, S.E. The bad taste of medicines: Overview of basic research on bitter taste. Clin. Ther. 2013, 35, 1225–1246. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rodrigo, C.; Ribas, L.; Serra-Majem, L.; Aranceta, J. Food preferences of spanish children and young people: The enKid Study. Eur. J. Clin. Nutr. 2003, 57 (Suppl. 1), S45–S48. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. Taste preferences and food intake. Ann. Rev. Nutr. 1997, 17, 237–253. [Google Scholar] [CrossRef]
- Ross, S. ‘Do I really have to eat that?’: A qualitative study of schoolchildren’s food choices and preferences. Health Educ. J. 1995, 54, 312–321. [Google Scholar] [CrossRef]
- Matsuzuki, H.; Muto, T.; Haruyama, Y. School children’s salt intake is correlated with salty taste preference assessed by their mothers. Tohoku J. Exp. Med. 2008, 215, 71–77. [Google Scholar] [CrossRef]
- Lioret, S.; McNaughton, S.A.; Spence, A.C.; Crawford, D.; Campbell, K.J. Tracking of dietary intakes in early childhood: The Melbourne InFANT program. Eur. J. Clin. Nutr. 2013, 67, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The Cardiovascular Risk in Young Finns Study. Br. J. Nutr. 2007, 93, 923. [Google Scholar] [CrossRef]
- Leyvraz, M.; Chatelan, A.; da Costa, B.R.; Taffe, P.; Paradis, G.; Bovet, P.; Bochud, M.; Chiolero, A. Sodium intake and blood pressure in children and adolescents: A systematic review and meta-analysis of experimental and observational studies. Int. J. Epidemiol. 2018, 47, 1796–1810. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Lichtenstein, A.H.; Callahan, E.A.; Sinaiko, A.; Van Horn, L.; Whitsel, L. Reducing sodium intake in children: A public health investment. J. Clin. Hypertens (Greenwich) 2015, 17, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; He, F.J.; Nowson, C.A. 24-h urinary sodium excretion is associated with obesity in a cross-sectional sample of Australian schoolchildren. Br. J. Nutr. 2016, 115, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Pollock, N.K.; Kotak, I.; Gutin, B.; Wang, X.; Bhagatwala, J.; Parikh, S.; Harshfield, G.A.; Dong, Y. Dietary sodium, adiposity, and inflammation in healthy adolescents. Pediatrics 2014, 133, e635–e642. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.L.; Dunford, E.K.; Neal, B.C. A systematic survey of the sodium contents of processed foods. Am. J. Clin. Nutr. 2010, 91, 413–420. [Google Scholar] [CrossRef]
- Liem, D.G.; Miremadi, F.; Keast, R.S. Reducing sodium in foods: The effect on flavor. Nutrients 2011, 3, 694–711. [Google Scholar] [CrossRef]
- Keast, R.S.J.; Dalton, P.H.; Breslin, P.A.S. Flavour Interactions at the Sensory Level. In Flavour Preception; Blackwell Publishing: Oxford, UK, 2004. [Google Scholar]
- Cruz, A.G.; Faria, J.A.F.; Pollonio, M.A.R.; Bolini, H.M.A.; Celeghini, R.M.S.; Granato, D.; Shah, N.P. Cheeses with reduced sodium content: Effects on functionality, public health benefits and sensory properties. Trends Food Sci. Technol. 2011, 22, 276–291. [Google Scholar] [CrossRef]
- Desmond, E. Reducing salt: A challenge for the meat industry. Meat. Sci. 2006, 74, 188–196. [Google Scholar] [CrossRef]
- Keast, R.S.J.; Breslin, P.A.S. An overview of binary taste-taste interactions. Food Qual. Prefer. 2002, 14, 111–124. [Google Scholar] [CrossRef]
- Hutton, T. Sodium: Technological functions of salt in the manufacturing of food and drink products. Br. Food J. 2002, 104, 126–152. [Google Scholar] [CrossRef]
- Bouhlal, S.; Chabanet, C.; Issanchou, S.; Nicklaus, S. Salt content impacts food preferences and intake among children. PLoS ONE 2013, 8, e53971. [Google Scholar] [CrossRef] [PubMed]
- Leshem, M. Biobehavior of the human love of salt. Neurosci. Biobehav. Rev. 2009, 33, 1–17. [Google Scholar] [CrossRef]
- Shepherd, R.; Farleigh, C.A.; Land, D.G. Preference and sensitivity to salt taste as determinants of salt-intake. Appetite 1984, 5, 187–197. [Google Scholar] [CrossRef]
- Lucas, L.; Riddell, L.; Liem, G.; Whitelock, S.; Keast, R. The influence of sodium on liking and consumption of salty food. J. Food Sci. 2011, 76, S72–S76. [Google Scholar] [CrossRef] [PubMed]
- Bertino, M.; Beauchamp, G.K.; Engelman, K. Long-term reduction in dietary sodium alters the taste of salt. Am. J. Clin. Nutr. 1982, 36, 1134–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blais, C.A.; Pangborn, R.M.; Borhani, N.O.; Ferrell, M.F.; Prineas, R.J.; Laing, B. Effect of dietary sodium restriction on taste responses to sodium chloride: A longitudinal study. Am. J. Clin. Nutr. 1986, 44, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Bertino, M.; Beauchamp, G.K. Increasing dietary salt alters salt taste preference. Physiol. Behav. 1986, 38, 203–213. [Google Scholar] [CrossRef]
- James, C.E.; Laing, D.G.; Oram, N. A comparison of the ability of 8–9-year-old children and adults to detect taste stimuli. Physiol. Behav. 1997, 62, 193–197. [Google Scholar] [CrossRef]
- Cowart, B.J.; Beauchamp, G.K. The Importance of Sensory Context in Young Children’s Acceptance of Salty Tastes. Child. Dev. 1986, 57, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Bolhuis, D.P.; Gijsbers, L.; de Jager, I.; Geleijnse, J.M.; de Graaf, K. Encapsulated sodium supplementation of 4weeks does not alter salt taste preferences in a controlled low sodium and low potassium diet. Food Qual. Preference 2015, 46, 58–65. [Google Scholar] [CrossRef]
- James, W.P.T.; Ralph, A.; Sanchez-Castillo, C.P. The dominance of salt in manufactured food in the sodium intake of affluent societies. Lancet 1987, 329, 426–428. [Google Scholar] [CrossRef]
- Grimes, C.A.; Booth, A.; Khokhar, D.; West, M.; Margerison, C.; Campbell, K.; Nowson, C. The Development of a Web-Based Program to Reduce Dietary Salt Intake in Schoolchildren: Study Protocol. JMIR Res. Protoc. 2017, 6, e103. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Booth, A.; Khokhar, D.; West, M.; Margerison, C.; Campbell, K.J.; Nowson, C.A. Digital Education to Limit Salt in the Home (DELISH) Program Improves Knowledge, Self-Efficacy, and Behaviors Among Children. J. Nutr. Educ. Behav. 2018, 50, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Baxter, J.R.; Campbell, K.J.; Riddell, L.J.; Rigo, M.; Liem, D.G.; Keast, R.S.; He, F.J.; Nowson, C.A. Cross-sectional study of 24-Hour urinary electrolyte excretion and associated health outcomes in a convenience sample of Australian primary schoolchildren: The Salt and Other Nutrients in Children (SONIC) study protocol. JMIR Res. Protoc. 2015, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Reducing Salt Intake in Populations. Report of a WHO Forum and Technical Meeting; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Chloride and Sulfate; Institute of Medicine: Washington, DC, USA, 2004. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1–6. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef]
- Grimes, C.A.; Campbell, K.J.; Riddell, L.J.; Nowson, C.A. Sources of sodium in Australian children’s diets and the effect of the application of sodium targets to food products to reduce sodium intake. Br. J. Nutr. 2011, 105, 468–477. [Google Scholar] [CrossRef]
- Birch, L.L. Dimensions of preschool children’s food preferences. J. Nutr. Educ. 1979, 11, 77–80. [Google Scholar] [CrossRef]
- Liem, D.G.; Mennella, J.A. Heightened sour preferences during childhood. Chem. Senses 2003, 28, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Bobowski, N.; Rendahl, A.; Vickers, Z. Preference for salt in a food may be alterable without a low sodium diet. Food Qual. Preference 2015, 39, 40–45. [Google Scholar] [CrossRef]
- Girgis, S.; Neal, B.; Prescott, J.; Prendergast, J.; Dumbrell, S.; Turner, C.; Woodward, M. A one-quarter reduction in the salt content of bread can be made without detection. Eur. J. Clin. Nutr. 2003, 57, 616–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.J.; Brinsden, H.C.; MacGregor, G.A. Salt reduction in the United Kingdom: A successful experiment in public health. J. Hum. Hypertens 2014, 28, 345–352. [Google Scholar] [PubMed]
- Institute of Medicine. Strategies to Reduce Sodium Intake in the United States; The National Academic Press: Washington, DC, USA, 2010. [Google Scholar]
- Khokhar, D.; Nowson, C.; Margerison, C.; West, M.; Campbell, K.; Booth, A.; Grimes, C. The Digital Education to Limit Salt in the Home Program Improves Salt-Related Knowledge, Attitudes, and Behaviors in Parents. J. Med. Internet Res. 2018, forthcoming/in press. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Food Item | Sodium (mg) | Salt Equiv. (g) | Energy (kJ) | Sugars (g) | Total Fat (g) |
|---|---|---|---|---|---|
| Potato chips | |||||
| No added salt | 14.0 | 0.04 | 2120.0 | 0.3 | 24.4 |
| Mid salt | 200.0 | 0.5 | 2200.0 | 0.3 | 30.0 |
| High salt | 486.0 | 1.2 | 2090.0 | 0.0 | 27.0 |
| Corn flakes | |||||
| Low salt | 90.0 | 0.2 | 1510.0 | 6.0 | 2.0 |
| Mid salt | 390.0 | 1.0 | 1580.0 | 4.9 | 0.7 |
| High salt | 590.0 | 1.5 | 1520.0 | 8.6 | 0.3 |
| N | Proportion (%) | Mean | SD | |
|---|---|---|---|---|
| Sex | ||||
| Male | 40 | 44 | ||
| Female | 52 | 56 | ||
| Age | 9.09 | 0.78 | ||
| BMI category * | ||||
| Healthy weight | 73 | 79 | ||
| Overweight | 12 | 13 | ||
| Obese | 7 | 8 | ||
| SES ** | ||||
| Low | 21 | 26 | ||
| Mid | 26 | 32 | ||
| High | 35 | 43 | ||
| Sodium intake (mmol) *** | 91 | 41 | ||
| Salt intake (g) *** | 5.35 | 2.43 |
| Potato Chips | Corn Flakes | |||||||
|---|---|---|---|---|---|---|---|---|
| Salt content | T1 (n = 92) | T2 (n = 76) | T1 (n = 90) * | T2 (n = 76) | ||||
| n | % | n | % | n | % | n | % | |
| Low/no salt | 22 | 24 | 18 | 24 | 3 | 3 | 15 | 20 |
| Mid salt | 27 | 29 | 24 | 32 | 32 | 36 | 19 | 25 |
| High salt | 43 1 | 47 | 34 2 | 45 | 55 3 | 61 | 41 4 | 55 |
| Potato Chips | Corn Flakes | |||||||
|---|---|---|---|---|---|---|---|---|
| Salt content | T1 (n = 92) | T2 (n = 76) | T1 (n = 92) | T2 (n = 76) | ||||
| n | % | n | % | n | % | n | % | |
| Low/no salt | 2 | 2 | 4 | 5 | 15 | 16 | 12 | 16 |
| Mid salt | 38 | 41 | 35 | 46 | 19 | 21 | 17 | 22 |
| High salt | 52 1 | 57 | 37 2 | 49 | 58 3 | 63 | 47 4 | 62 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
West, M.; Liem, D.G.; Booth, A.; Nowson, C.; Grimes, C. Salt Preference and Ability to Discriminate between Salt Content of Two Commercially Available Products of Australian Primary Schoolchildren. Nutrients 2019, 11, 388. https://doi.org/10.3390/nu11020388
West M, Liem DG, Booth A, Nowson C, Grimes C. Salt Preference and Ability to Discriminate between Salt Content of Two Commercially Available Products of Australian Primary Schoolchildren. Nutrients. 2019; 11(2):388. https://doi.org/10.3390/nu11020388
Chicago/Turabian StyleWest, Madeline, Djin Gie Liem, Alison Booth, Caryl Nowson, and Carley Grimes. 2019. "Salt Preference and Ability to Discriminate between Salt Content of Two Commercially Available Products of Australian Primary Schoolchildren" Nutrients 11, no. 2: 388. https://doi.org/10.3390/nu11020388