Associations of Maternal Vitamin D Deficiency with Pregnancy and Neonatal Complications in Developing Countries: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Criteria
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
3. Results
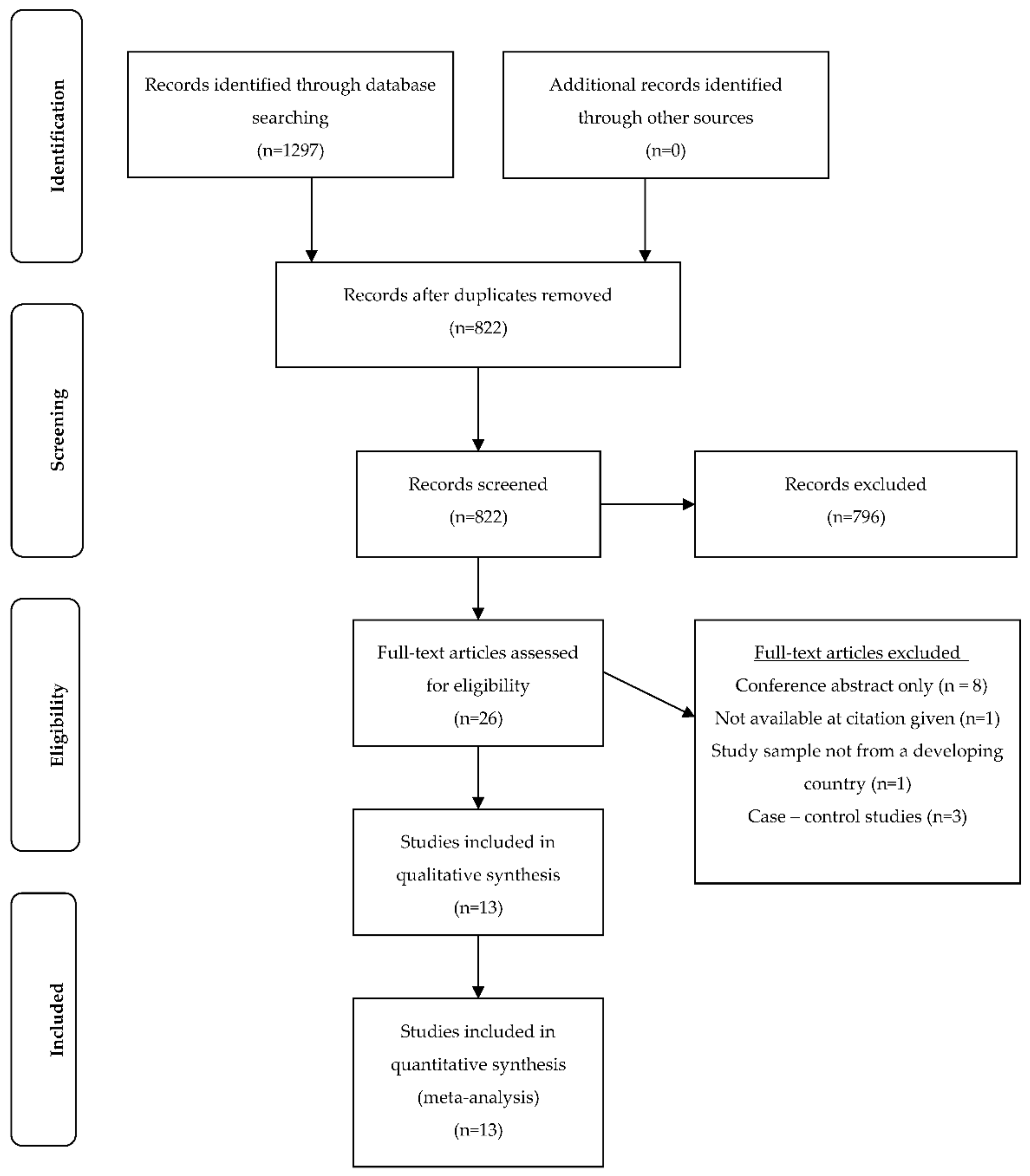
3.1. Study Selection
3.2. Setting and Participants
3.3. Vitamin D Assessment
3.4. Vitamin D Deficiency, Criteria and Prevalence
3.5. Maternal and Neonatal Outcomes
3.6. Biological and Lifestyle Risk Factors
3.7. Study Quality
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [PubMed]
- Kiely, M.E. Invited commentray: Further evidence that prevention of maternal vitamin D deficiency may benefit the health of the next generation. Br. J. Nutr. Diet. 2016, 116, 573–575. [Google Scholar]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global consensus recommendations on prevention and management of nutritional rickets. Hormone Res. Paediatr. 2016, 85, 83–106. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Vitamin D. Vitamin and Mineral Requirements in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation, 2nd ed.; WHO: Geneva, Switzerland, 2003; Chapter 3. [Google Scholar]
- Toko, E.N.; Sumba, O.P.; Daud, I.I.; Ogolla, S.; Majiwa, M.; Krisher, J.T.; Ouma, C.; Dent, A.E.; Rochford, R.; Mehta, S. Maternal vitamin D status and adverse birth outcomes in children from rural western Kenya. Nutrients 2016, 8, 794. [Google Scholar] [CrossRef] [PubMed]
- Nimitphong, H.; Holick, M.F. Vitamin D status and sun exposure in southeast Asia. Derm. Endocrinol. 2013, 5, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Spiegelman, D.; Aboud, S.; Giovannucci, E.L.; Msamanga, G.I.; Hertzmark, E.; Mugusi, F.M.; Hunter, D.J.; Fawzi, W.W.; Mehta, S.; et al. Lipid-soluble vitamins A, D, and E in HIV-infected pregnant women in Tanzania. Eur. J. Clin. Nutr. 2010, 64, 808–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halicioglu, O.; Aksit, S.; Koc, F.; Akman, S.A.; Albudak, E.; Yaprak, I.; Coker, I.; Colak, A.; Ozturk, C.; Gulec, E.S. Vitamin D deficiency in pregnant women and their neonates in spring time in western Turkey. Paediatr. Perinat. Epidemiol. 2012, 26, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Smith, J.R.; Philipp, B.L.; Chen, T.C.; Mathieu, J.; Holick, M.F. Vitamin D deficiency in a healthy group of mothers and newborn infants. Clin. Pediatr. 2007, 46, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, N.; Esra, H.; Begum, A.; Fatma, D.; Arzu, Y.; Yalcin, H.; Fatih, K.; Selahattin, K. Relation of maternal vitamin D status with gestational diabetes mellitus and perinatal outcome. Afr. Health Sci. 2015, 15, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Tao, M.; Shao, H.; Gu, J.; Zhen, Z. Vitamin D status of pregnant women in Shanghai, China. J. Matern. Fetal Neonatal Med. 2012, 25, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; De-Regil, L.M.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation during pregnancy: Updated meta-analysis on maternal outcomes. J. Steroid Biochem. Mol. Biol. 2016, 164, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Verstuyf, A.; Carmeliet, G.; Bouillon, R.; Mathieu, C. Vitamin D: A pleiotropic hormone. Kidney Int. 2010, 78, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Strugnell, S.A.; DeLuca, H.F. Current understanding of the molecular actions of vitamin D. Physiol. Rev. 1998, 78, 1193–1231. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Qi, H.P.; Luo, Z.C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Lapillonne, A. Vitamin D deficiency during pregnancy may impair maternal and fetal outcomes. Med. Hypotheses 2010, 74, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Josefson, J.L.; Reisetter, A.; Scholtens, D.M.; Price, H.E.; Metzger, B.E.; Langman, C.B.; Group HSCR. Maternal BMI associations with maternal and cord blood vitamin D levels in a North American subset of hyperglycemia and adverse pregnancy outcome (HAPO) study participants. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.; Whitehouse, A.J.O.; Newnham, J.P.; Gorman, S.; Jacoby, P.; Holt, B.J.; Serralha, M.; Tearne, J.E.; Holt, P.G.; Hart, P.H.; et al. Low maternal serum vitamin D during pregnancy and the risk for postpartum depression symptoms. Arch. Women’s Ment. Health 2014, 17, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.; Jarjou, L.M.A.; Goldberg, G.R.; Bennett, J.; Cole, T.J.; Schoenmakers, I. Maternal plasma 25-hydroxyvitamin D concentration and birthweight, growth and bone mineral accretion of Gambian infants. Acta Paediatr. 2009, 98, 1360–1362. [Google Scholar] [CrossRef] [PubMed]
- Eggemoen, Å.R.; Falk, R.S.; Knutsen, K.V.; Lagerløv, P.; Sletner, L.; Birkeland, K.I.; Jenum, A.K. Vitamin D deficiency and supplementation in pregnancy in a multiethnic population-based cohort. BMC Pregnancy Child. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Lips, P.; van Schoor, N.M.; de Jongh, R.T. Diet, sun, and lifestyle as determinants of vitamin D status. Ann. N. Y. Acad. Sci. 2014, 1317, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Ferguson, E.L.; Penrose, K.; Arimond, M. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. J. Nutr. 2010, 140, 2051S–2058S. [Google Scholar] [CrossRef] [PubMed]
- Ajmani, S.N.; Paul, M.; Chauhan, P.; Ajmani, A.K.; Yadav, N. Prevalence of vitamin D deficiency in burka-clad pregnant women in a 450-bedded maternity hospital of Delhi. J. Obs. Gynecol. India 2016, 66, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Pirdehghan, A.; Vakili, M.; Dehghan, R.; Zare, F. High prevalence of vitamin D deficiency and adverse pregnancy outcomes in Yazd, a central province of Iran. J. Reprod. Infertil. 2016, 17, 34–38. [Google Scholar] [PubMed]
- Song, S.; Si, S.; Liu, J.; Chen, X.; Zhou, L.; Jia, G.; Liu, G.; Niu, Y.; Wu, J.; Zhang, W. Vitamin D status in Chinese pregnant women and their newborns in Beijing and their relationships to birth size. Public Health Nutr. 2013, 16, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Gbadegesin, A.; Sobande, A.; Adedeji, O.; Disu, E.; Korede, O.; Dosunmu, A.; Shakunle, A. Maternal serum vitamin D levels and pregnancy outcomes: From Lagos, Nigeria. J. Obs. Gynaecol. 2017, 37, 25–28. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Cohort and case control studies. In Special Programme of Research, Development and Research Training in Human Reproduction; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Lewallen, S.; Courtright, P. Epidemiology in practice: Case-control studies. Commun. Eye Health 1998, 11, 57–58. [Google Scholar]
- Fatusi, A.O. Young people’s sexual and reproductive health interventions in developing countries: Making the investments count. J. Adolesc. Health 2016, 59, S1–S3. [Google Scholar] [CrossRef] [PubMed]
- Department of Foreign Affairs and Trade (DFAT). List of Developing countries as declared by the Minister for Foreign Affairs; DFAT: Canberra, Australia, 2015.
- Van der Pligt, P.; Willcox, J.; Hesketh, K.D.; Ball, K.; Wilkinson, S.; Crawford, D.; Campbell, K. Systematic review of lifestyle interventions to limit postpartum weight retention: Implications for future opportunities to prevent maternal overweight and obesity following childbirth. Obes. Rev. 2013, 14, 792–805. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H. Quality assessment tool for quantitative studies. In Effective Public Health Practice Project; McMaster University: Toronto, ON, Canada, 2003. [Google Scholar]
- Farrant, H.J.W.; Krishnaveni, G.V.; Hill, J.C.; Boucher, B.J.; Fisher, D.J.; Noonan, K.; Osmond, C.; Veena, S.R.; Fall, C.H.D. Vitamin D insufficiency is common in Indian mothers but is not associated with gestational diabetes or variation in newborn size. Eur. J. Clin. Nutr. 2009, 63, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-H.; Fu, L.; Hao, J.-H.; Yu, Z.; Zhu, P.; Wang, H.; Xu, Y.-Y.; Zhang, C.; Tao, F.-B.; Xu, D.-X. Maternal vitamin D deficiency during pregnancy elevates the risks of small for gestational age and low birth weight infants in Chinese population. J. Clin. Endocrinol. Metab. 2015, 100, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Xin, Z.; Jianping, X.; Rui, F.; Renqiang, Y.; Daozhen, C.; Jun, Z. Maternal vitamin D status in the late second trimester and the risk of severe preeclampsia in southeastern China. Nutrients 2017, 9, 138. [Google Scholar] [CrossRef]
- Ates, S.; Sevket, O.; Ozcan, P.; Ozkal, F.; Kaya, M.O.; Dane, B. Vitamin D status in the first-trimester: Effects of vitamin D deficiency on pregnancy outcomes. Afr. Health Sci. 2016, 16, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Aydogmus, S.; Kelekci, S.; Aydogmus, H.; Eriş, S.; Desdicioğlu, R.; Yilmaz, B.; Sağlam, G. High prevalence of vitamin D deficiency among pregnant women in a Turkish population and impact on perinatal outcomes. J. Matern. Fetal Neonatal Med. 2015, 28, 1828–1832. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Kanani, F.H.; Ramzan, S.; Kausar, R.; Ayaz, S.; Khanani, R.; Pal, L. Obstetric and neonatal outcomes of maternal vitamin d supplementation: Results of an open-label, randomized controlled trial of antenatal vitamin d supplementation in pakistani women. J. Clin. Endocrinol. Metab. 2014, 99, 2448–2455. [Google Scholar] [CrossRef] [PubMed]
- Maghbooli, Z.; Hossein-Nezhad, A.; Karimi, F.; Shafaei, A.-R.; Larijani, B. Correlation between vitamin D3 deficiency and insulin resistance in pregnancy. Diabetes Metab. Res. Rev. 2008, 24, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Gur, E.B.; Gokduman, A.; Turan, G.A.; Tatar, S.; Hepyilmaz, I.; Zengin, E.B.; Eskicioglu, F.; Guclu, S. Mid-pregnancy vitamin D levels and postpartum depression. Eur. J. Obs. Gynecol. Reprod. Biol. 2014, 179, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Khanani, R.; Hussain-Kanani, F.; Tahira, S.; Shaheen, A.; Pal, L. High prevalence of vitamin D deficiency in Pakistani mothers and their newborns. Int. J. Gynecol. Obs. 2011, 112, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Saraf, R.; Morton, S.M.B.; Camargo, C.A.; Grant, C.C. Global summary of maternal and newborn vitamin D status—A systematic review. Matern. Child Nutr. 2016, 12, 647–668. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Levin, C.; Walker, N.; Chou, D.; Liu, L.; Temmerman, M. Reproductive, maternal, newborn, and child health: Key messages from Disease Control Priorities 3rd Edition. Lancet 2016, 388, 2811–2824. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. Br. Med. J. 2013, 346. [Google Scholar] [CrossRef] [PubMed]
- Umesawa, M.; Kobashi, G. Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertens. Res. 2016, 40, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bertozzi-Villa, A.; Coggeshall, M.S.; Shackelford, K.A.; Steiner, C.; Heuton, K.R.; Gonzalez-Medina, D.; Barber, R.; Huynh, C.; Dicker, D.; et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 980–1004. [Google Scholar] [CrossRef]
- World Health Organisation. Vitamin D supplementation during pregnancy for the prevention of pre-eclampsia. In e-Library of Evidence for Nutrition Actions (eLENA); WHO: Geneva, Switzerland, 2016. [Google Scholar]
- The United Nations. Sustainable Development Goals Report; The United Nations: New York, NY, USA, 2017. [Google Scholar]
- The United Nations. Sustainable Development Goals: 17 Golas to Transform Our World; The United Nations: New York, NY, USA, 2015. [Google Scholar]
- Global nutrition report: Tracking progress, strengthening accountability, reducing malnutrition faster. In Nourishing the SDGs; Development Initiatives: Bristol, UK, 2017.
- World Health Organisation. Exclusive Breastfeeding for Six Motnhs Best for Babies Everywhere; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Takeuchi, A.; Okano, T.; Tsugawa, N.; Tasaka, Y.; Kobayashi, T.; Kodama, S.; Matsuo, T. Effects of ergocalciferol supplementation on the concentration of vitamin D and its metabolites in human milk. J. Nutr. 1989, 119, 1639–1646. [Google Scholar] [CrossRef] [PubMed]
- Saadi, H.F.; Dawodu, A.; Afandi, B.O.; Zayed, R.; Benedict, S.; Nagelkerke, N. Efficacy of daily and monthly high-dose calciferol in vitamin D–deficient nulliparous and lactating women. Am. J. Clin. Nutr. 2007, 85, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Nozza, J.M.; Rodda, C.P. Vitamin D deficiency in mothers of infants with rickets. Med. J. Aust. 2001, 175, 253–255. [Google Scholar] [PubMed]
- Elder, C.J.; Bishop, N.J. Rickets. Lancet 2014, 383, 1665–1676. [Google Scholar] [CrossRef]
- Baker, R.D.; Greer, F.R. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age). Pediatrics 2010, 126, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Taren, D.; Lutter, C.K. The role of breastfeeding protection, promotion and support in a developing world. In Nutrition and Health in a Developing World; de Pee, S., Taren, D., Bloem, M.W., Eds.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Davies-Tuck, M.; Yim, C.; Knight, M.; Hodges, R.; Doery, J.C.; Wallace, E. Vitamin D testing in pregnancy: Does one size fit all? Aust. N. Z. J. Obstet. Gynaecol. 2015, 55, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Christesen, H.T.; Elvander, C.; Lamont, R.F.; Jorgensen, J.S. The impact of vitamin D in pregnancy on extraskeletal health in children: A systematic review. Acta Obstet. Gynecol. Scand. 2012, 91, 1368–1380. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Anagnostis, P.; Paschou, S.A.; Kandaraki, E.; Goulis, D.G. Vitamin D status during pregnancy: Time for a more unified approach beyond borders? Eur. J. Clin. Nutr. 2015, 69, 874–877. [Google Scholar] [CrossRef] [PubMed]
- Arneson, W.L.; Arneson, D.L. Current methods for routine clinical laboratory testing of Vitamin D levels. Lab. Med. 2013, 44, e38–e42. [Google Scholar] [CrossRef]
- Sempos, C.T.; Vesper, H.W.; Phinney, K. Vitamin D Standardization Program (VDSP). Available online: https://ods.od.nih.gov/Research/vdsp.aspx (accessed on 17 May 2018).
- World Health Organisation. Vitamin D supplementation during pregnancy: Guidance summary. In e-Library of Evidence for Nutrition Actions (eLENA); WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Veselka, B.; van der Merwe, A.E.; Hoogland, M.L.P.; Waters-Rist, A.L. Gender-related vitamin D deficiency in a Dutch 19th century farming community. Int. J. Paleopathol. 2017. [Google Scholar] [CrossRef]


{kind=link}
| Study | Design | Recruitment | Sample | Serum Vitamin D Measurement | Criteria for Vitamin D Deficiency and Reported Prevalence | Outcomes | Risk Factors |
|---|---|---|---|---|---|---|---|
| Ajmani et al., 2016 India [24] | Prospective cohort | Approached/screened: not reported Enrolled: not reported Complete data: n = 200 burka-clad women Setting: antenatal clinic and inpatients in antenatal ward at Kasturba Hospital, Delhi Season: all (year-long) | Age: mean 24.8 years Demographics: 64.5% multigravida, 44% dark complexion, 36% low SES, 64% illiterate, 2.5% graduate level educated Trimester: not reported Exclusion criteria: non-burka clad, age <18 years or >40 years, history of liver/renal disease, osteoporosis or rheumatoid arthritis, antitubercular or antiepileptic treatment in last 6 months, taking vitamin D supplements | ELISA | Criteria *: Deficiency < 50 nmol/L Inadequacy 50–75 nmol/L Adequate > 75 nmol/L Prevalence of deficiency: Deficient n = 75 (37.5%) Inadequate n = 78 (39%) Adequate n = 47 (23.5%) | Maternal: 7.5% women diagnosed with pre-eclampsia, significant correlation between VDD and pre-eclampsia (p = 0.001) Neonatal: 9.5% LBW babies, significant correlation between VDD and LBW (p = 0.0001) No correlation: VDD and GDM, LSCS, bony abnormality, Apgar score, premature birth or NICU admission | Dark skin complexion, limited outdoor activity, low dairy intake, low fish intake (p < 0.05) |
| Ates et al., 2016 Turkey [37] | Prospective cohort | Approached/screened: n = 286 Enrolled: n = 266 (93%) Complete data: n = 229 (86%) Setting: first antenatal appointment at outpatient clinic of Obstetrics and Gynecology, Bezmialem Vakif University, Istanbul Season: 48.9% summer (May–October), 51.1% winter (November–April) | Age: mean 29.5 years Demographics: 64.5% primigravida, mean BMI 25.3 kg/m2, 61.3% covered dress, 63.1% multivitamin use, 6.6% smoking, 46.9% ≥ 9 years education Trimester: first Exclusion criteria: thyroid, parathyroid or adrenal disease, hepatic or renal failure, metabolic bone disease, medication affecting vitamin D metabolism, multiple pregnancy, taking vitamin D supplements | LC-MS/MS | Criteria *: Severe deficiency < 25 nmol/L Mod deficiency 25–47.5 nmol/L Mild deficiency 50–72.5 nmol/L Adequate > 75 nmol/L Prevalence of deficiency: Severe n = 105 (45.9%) Mod n = 83 (36.2%) Mild n = 31 (13.5%) Adequate n = 10 (4.4%) | Maternal: 53.8% women with severe VDD had vaginal delivery, compared with 32.7% as primary caesarean section (p = 0.018) No correlation: VDD and GDM, pre-eclampsia, gestational hypertension, preterm birth, SGA, intrauterine fetal death, congenital malformation, birth weight or Apgar score | Covered dress, non-multivitamin use, winter (p < 0.05) |
| Aydogmus et al., 2014 Turkey [38] | Prospective cohort | Approached/screened: n = 180 Enrolled: n = 152 (84%) Complete data: n = 148 (97%) Setting: inpatients at Izmir Katip Celebi University Ataturk Training and Research Hospital, Izmir Season: not reported | Age: mean 24.4 years Demographics: not reported Trimester: third Exclusion criteria: taking vitamin D supplements, multiparity, disease affecting vitamin D and calcium metabolism, medications for chronic disease | ELISA | Criteria *: Deficient < 37.5 nmol/L Insufficient 37.5–72.5 nmol/L Sufficient > 75 nmol/L (grouped for analysis Deficient < 37.5 nmol/L; Other ≥ 37.5 nmol/L) Prevalence of deficiency: Deficient: n = 66 (44.6%) Other n = 82 (55.4%) | Maternal: 39.9% women with VDD had poor pregnancy outcomes compared with 23.2% of women without VDD (p = 0.001), VDD increased risk of perinatal complications (OR 4.30; 95% CI 1.85–9.99) Neonatal: 16.7% SGA neonates born to mothers with VDD compared with 4.9% neonates born to mothers without VDD (p = 0.007), VDD increased risk of SGA (OR 4.5; 95% CI 1.41–15.78); mean birthweight significantly lower for neonates born to mothers with VDD (3187.6 ± 495.5 g) compared with those born to mothers without VDD (3268.1 ± 477.1 g) (p = 0.02) No correlation: VDD and mode of delivery, post maturity, GDM, maternal anemia, hypertension, pre-eclampsia, cholestasis, oligohydraminos, fetal distress, still birth, preterm labor, PPROM, Apgar scores, prolonged hospitalization, mortality, NICU admission or macrosomia | No significant associations |
| Chen et al., 2015 China [35] | Prospective cohort | Approached/screened: n = 4358 (sub-sample of a population-based cohort study n = 16,766) Enrolled: n = 3658 (84%) Complete data: 3658 (100%) Setting: women recruited to the larger China-Anhui Birth Cohort study from six major cities of Anhui province Season: all (year-long), 36.7% spring, 22.5% summer, 20.6% autumn, 20.2% winter | Age: mean 27.5 years Demographics: 96.0% nulliparous, 45.2% low income, 75.3% healthy BMI, 16.5% multivitamin use Trimester: all, 35.1% first, 62.0% second, 2.9% third Exclusion criteria: multiple pregnancy, abortion | RIA | Criteria *: Deficient < 50 nmol/L Insufficient 50–74.75 nmol/L Sufficient ≥ 75 nmol/L Prevalence of deficiency: Deficiency n = 1405 (38.4%) Insufficiency n = 1289 (35.2%) Sufficient n = 964 (26.4%) | Maternal: not assessed Neonatal: 16.01% SGA neonates born to mothers with VDD compared with 5.59% born to mothers with vitamin D insufficiency and 2.80% with sufficient vitamin D (p < 0.001); compared to sufficiency, maternal VDD increased risk of SGA (RR 6.47; 95% CI 4.30–9.75) and insufficiency (RR 2.01; 95% CI 1.28–3.16) (p < 0.001); 4.98% LBW neonates born to mothers with VDD compared with 1.32% born to mothers with vitamin D insufficiency and 0.41% with sufficient vitamin D (p < 0.001); VDD increased risk of LBW (RR 12.31; 95% CI 4.47–33.89) (p < 0.001). Adjusted for: Pre-pregnancy maternal BMI, maternal age, season and gestational week | Not assessed |
| Farrant et al., 2009 India [34] | Prospective cohort | Approached/screened: n = 1539 Enrolled: n = 830 (54%) Complete data: n = 674 (81%) Setting: women attending antenatal clinic at Holdsworth Memorial Hospital, Mysore Season: all (year-long) | Age: mean 23.7 years Demographics: mean BMI 23.4 kg/m2, women supplemented at recruitment (n = 156) with vitamin D as part of routine management, no information available at 30 weeks Trimester: third Exclusion criteria: not reported | RIA | Criteria: Hypovitaminosis < 50 nmol/L Adequate > 50 nmol/L Prevalence of deficiency: Hypovitaminosis n = 372 (67%) Adequate: n = 187 (33%) | No correlation: VDD and GDM, birthweight, impaired fetal growth | Autumn/winter (p < 0.05) |
| Gbadegesin et al., 2016 Nigeria [27] | Prospective cohort | Approached/screened: not reported Enrolled: n = 461 Complete data: n = 461 (100%) Setting: maternity unit of the Lagos State University Teaching Hospital, Ikeja and women of mixed ethnicity, social class and religion Season: all (year-long) | Age: mean 31.3 years Demographics: mean parity 1.16 Trimester: all Exclusion criteria: multiple pregnancy, previous medical condition (hypertension, renal disease, diabetes), taking vitamin D supplements, elevated BP | HPLC | Criteria *: Deficiency < 50 nmol/L Insufficiency 52.5–75 nmol/L Adequate > 75 nmol/L Prevalence of deficiency: Deficiency n = 134 (29.0%) Insufficiency n = 48 (10.4%) Adequate n = 279 (60.6%) | No correlation: VDD and preeclampsia, SROM, anemia, GDM, preterm delivery, mode of delivery, Apgar score or stillbirth | No significant associations |
| Gur et al., 2014 Turkey [41] | Prospective cohort | Approached/screened: n = 687 Enrolled: n = 208 (30%) Complete data: n = 189 at 1/52 (91%); n = 184 at 6/52 (88%); n = 179 at 6/12 (86%) Setting: women attending routine antenatal reviews at Sifa University Bornova Health Research and Application Hospital, Izmir Season: summer/autumn | Age: mean 28.5 years Demographics: mean BMI 26.5 kg/m2, 7.6% women supplemented with vitamin D ≥ 3 days per week and 84.6% supplemented daily, all women Caucasian and native Turkish speaking Trimester: second Exclusion criteria: unmarried, unplanned pregnancy, BMI < 20 or >30 kg/m2, smoker, diagnosed psychiatric illness, pre-diagnosed medical condition, parity > 3, education level < 8 years, multiple birth, employed, annual income < US $450, fetal death, complex delivery, newborn with anomaly, postpartum bleeding or hysterectomy | ELISA | Criteria *: Severe deficiency < 25 nmol/L Mild deficiency 25 nmol/L–50 nmol/L Normal ≥ 50 nmol/L Prevalence of deficiency: Severe: n = 23 (11%) Mild n = 84 (40.3%) Normal n = 101 (48.5%) | Maternal: 21.1%, 23.2% and 23.7% women had PPD at week 1, 6 and 6 months respectively; significant negative correlation (r = −0.2, −0.2, −0.3) between vitamin D levels and Edinburgh Postnatal Depression Scale (EPDS) score at each of the three time points; mean vitamin D level was significantly different between women with and without PPD at each of the three time points (p = 0.003, p = 0.004 and p < 0.001 respectively) Neonatal: not assessed | Not assessed |
| Hossain et al., 2010 Pakistan [39] | Cross-sectional | Approached: not reported (all women admitted to the labor suite for delivery during the study period were deemed eligible) RR: not reported Complete data: n = 75 Setting: delivery at Dow University of Health Sciences and Civil Hospital, Karachi Season: spring | Age: mean 26.0 years Demographics: mean BMI 27 kg/m2, mean parity 2.2, 26% covering arms, hands heads, 76% covering face Trimester: third Exclusion criteria: not reported | CI | Criteria *: Severe deficiency < 25 nmol/L Mod deficiency 27.5–50 nmol/L Mild deficiency 52.5–60 nmol/L Adequate > 60 nmol/L Prevalence of deficiency: Severe: n = 34 (45%) Mod: n = 20 (27%) Mild: n = 13 (17%) Adequate: n = 8 (11%) | Maternal: compared with women in the highest tertile for vitamin D, women in the lowest tertile and mid-tertile were more likely to meet criteria for pre-eclampsia and gestational pre-hypertension (OR 2.28; 95% CI 0.35–23.28) and (OR 19.27; 95% CI 1.96–188.92 respectively); vitamin D levels were inversely correlated with maternal mean arterial pressure (r = 0.029) (p = 0.020) Neonatal: not assessed in relation to maternal vitamin D Adjusted for maternal age, level of exercise, maternal weight, birthweight and gestational age | Not assessed |
| Maghbooli et al., 2008 Iran [40] | Cross-sectional | Approached/screened: not reported Enrolled: n = 741 Complete data: n = 579 Setting: referral to five university hospital clinics of the Tehran University of Medical Sciences during the first half of pregnancy Season: not reported | Age: mean 27.4 years Demographics: mean BMI 26.4 kg/m2 Trimester: second Exclusion criteria: prenatal diabetes | RIA | Criteria: Severe deficiency < 12.5 nmol/L Mild deficiency 12.5–24.9 nmol/L Mod deficiency 25–34.9 nmol/L Sufficiency > 34.9 nmol/L Prevalence of deficiency: Severe n = 201 (27.1%) Mild n = 118 (15.9%) Mod n = 344 (46.4%) Sufficient n = 78 (10.5%) | Maternal: 52% women diagnosed with GDM, mean vitamin D significantly lower in women with GDM (16.49 ± 10.44 nmol/L) compared with non-GDM women (22.97 ± 18.25 nmol/L) (p = 0.009), prevalence of severe VDD was significantly higher in women with GDM (44.2%) compared with non-GDM women (23.5%) (p = 0.011) Neonatal: not assessed | Not assessed |
| Pirdehghan et al., 2016 Iran [25] | Cross-sectional | Approached/screened: not reported Enrolled: not reported Complete data: n = 200 Setting: admission to hospital delivery room for natural delivery, caesarean section or abortion at Shahid Sadoughi hospital Season: autumn/spring | Age: mean 26.7 years Demographics: all women nulliparous, 48.7% diploma/university educated, 97.5% housewives, 38.5% women taking multivitamins containing vitamin D during pregnancy, Trimester: not reported Exclusion criteria: pre-existing medical conditions (renal or bone disorders), medication influencing calcium or vitamin D metabolism. multiparity | ELISA | Criteria *: Severe deficiency < 25 nmol/L Moderate deficiency 25–50 nmol/L Mild deficiency 52.5–75 nmol/L Adequate 75–125 nmol/L Upper normal/toxic > 125 nmol/L Prevalence of deficiency: (figures reported in text) Severe 12.5% Deficiency 60% | Maternal: mean vitamin D significantly higher in natural or elective caesarean section women compared with abortion and emergency caesarean section women (p = 0.040); VDD associated with risk of abortion 3.1 (1.39–6.8) which was higher in severe deficiency women compared with VDD women (p = 0.045), mean vitamin D significantly lower in women with oligohydramnios or polyhydramnios complication (13.9 + 9.5 and 20.6 + 10.8 respectively) (p = 0.045) No correlation: VDD and preeclampsia, PROM, GDM, birth weight, birth length, head circumference or Apgar score | No significant associations |
| Song et al., 2012 China [26] | Cross-sectional | Approached/screened: not reported Enrolled: not reported Complete data: 70 Setting: delivery at 306 Hospital of PLA in Beijing from surrounding communities of the Beijing urban area Season: spring | Age: 29.9 (±0.3) years Demographics: Mean weight: 73.9 kg, pregravid range 0–3 Trimester: third Exclusion criteria: multiparity, taking calcium and/or vitamin D supplements, pre-existing medical conditions (hypertension, renal disease, pre-gestational diabetes) | ELISA | Criteria: Severe deficiency < 25 nmol/L Mild deficiency 25– < 50 nmol/L Insufficiency 50– < 75 nmol/L (21–29 ng/mL) Sufficiency ≥ 75 nmol/L (grouped for analysis Deficient < 25 nmol/L and other ≥ 25 nmol/L Prevalence of deficiency: Severe n = 38 (54.5%) Mild n = 25 (35.7%) Insufficient n = 7 (10.0%) Sufficient n = 0 (0%) | Maternal: not assessed Neonatal: significant correlation between maternal vitamin D and newborn length (r = 0.247) (p = 0.039); compared with women who had vitamin D ≥ 25 nmol/L, birth weight (3633.1 g) and length (51.0 cm) of newborns were significantly lower in women with vitamin D < 25 nmol/L (3386 g and 50.2 cm respectively) (p = 0.015, p = 0.037) No correlation: VDD or head circumference | Not assessed |
| Toko et al., 2016 Kenya [6] | Longitudinal | Approached/screened: n = 99 RR: not reported Complete data: n = 63 (baseline data used) (64%) Setting: women residing within a 10 km radius of Chulaimbo Sub-district hospital in Kisumu County Season: dry season | Age: mean 22.5 years Demographics: mean BMI 22.9 kg/m2 Trimester: second and third Exclusion criteria: more than 26 weeks gestation, HIV infected, residing >10 km from the hospital | ELISA | Criteria: Deficiency < 50 nmol/L Insufficiency 50–75 nmol/L Sufficiency > 75 nmol/L (grouped for analysis low < 50 nmol/L and adequate ≥ 50 nmol/L) Prevalence of deficiency: Deficient n = 13 (20.6%) Insufficient n = 32 (50.8%) Sufficient n = 19 (28.6%) | Maternal: not assessed Neonatal: newborns more likely to have stunted growth at birth when born to mothers with deficient vitamin D (RR 4.4 (CI 1.0–18.6) (p = 0.04) and more likely to be born preterm (<37 weeks) (RR 5.4 (CI 1.1, 25.3) (p = 0.03) Adjusted for: maternal age, gestational age at delivery and maternal BMI No correlation: VDD and wasting or BMI z-score | Not assessed |
| Xin et al., 2017 China [36] | Prospective cohort | Approached/screened: not reported Enrolled: n = 13,806 Complete data: n = 11,151 (81%) Setting: routine visit to antenatal care clinic and delivery at the Wuxi Maternity and Child Health Hospital Season: 28.4% winter, 18.5% spring, 22.7% autumn, 30.4% summer | Age: mean 27.3 years Demographics: 88.9% nulliparous, 9.2% BMI ≥ 25 kg/m2, 96% GA at delivery ≥ 37 weeks Trimester: second and third Exclusion criteria: taking calcium and/or vitamin D supplements, pre-existing medical conditions (hypertension, renal disease, pre-gestational diabetes), fetal anomalies | CI | Criteria: Deficiency < 50 nmol/L Sufficiency > 50 nmol/L Prevalence of deficiency: Deficient n = 8799 (78.9%) Sufficient n = 2352 (20.8%) | Maternal: 1.2% pre-eclampsia, significant difference in incidence of severe pre-eclampsia in pregnant women with VDD (<50 nmol/L) (n = 123; 1.4%) compared with sufficiency (≥50 nmol/L) (n = 16; 0.6%) (p = 0.002), women with VDD were more at risk of developing severe pre-eclampsia compared with women who were vitamin D sufficient (OR: 3.16; 95% CI: 1.77–5.65) (p = 0.000) Adjusted for: pre-pregnancy BMI, maternal age, parity and season of blood sampling Neonatal: not assessed | Age ≥ 35 years, pre-pregnancy BMI ≥ 25 kg/m2, nulliparity (p < 0.05) |
| Maternal Outcomes | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | PE | GDM | Anemia | GHTN | OHD | Mode of Delivery * | Cholestasis | PPO | PH | MMAP | PPD | PC | PROM/SROM |
| Ajmani et al. (2016) India [24] | + | - | - | ||||||||||
| Ates et al. (2016) Turkey [37] | - | - | - | + | |||||||||
| Aydogmus et al. (2014) Turkey [38] | - | - | - | - | - | - | - | + | - | + | - | ||
| Chen et al. (2015) China [35] | |||||||||||||
| Farrant et al. (2009) India [34] | - | ||||||||||||
| Gbadegesin et al. (2016) Nigeria [27] | - | - | - | - | - | ||||||||
| Gur et al. (2014) Turkey [41] | + | ||||||||||||
| Hossain et al. (2010) Pakistan [39] | + | + | + | ||||||||||
| Maghbooli et al. (2008) Iran [40] | + | ||||||||||||
| Pirdehghan et al. (2016) Iran [25] | - | - | + | - | |||||||||
| Song et al. (2012) China [26] | |||||||||||||
| Toko et al. (2016) Kenya [6] | |||||||||||||
| Xin et al. (2017) China [36] | + | ||||||||||||
| Neonatal Outcomes | |||||||||||||
| Study | Macro. | Stunted Growth * | Preterm Birth | W z-Score | Still Birth/IFD | NICU Admit | Apgar Score | Post MB | HC | CM * | Birth Weight * | Birth Length | SGA |
| Ajmani et al. (2016) India [24] | - | - | - | - | + | ||||||||
| Ates et al. (2016) Turkey [37] | - | - | - | - | - | - | |||||||
| Aydogmus et al. (2014) Turkey [38] | - | - | - | - | - | - | + | + | |||||
| Chen et al. (2015) China [35] | + | + | |||||||||||
| Farrant et al. (2009) India [34] | - | - | |||||||||||
| Gbadegesin et al. (2016) Nigeria [27] | - | - | - | ||||||||||
| Gur et al. (2014) Turkey [41] | |||||||||||||
| Hossain et al. (2010) Pakistan [39] | |||||||||||||
| Maghbooli et al. (2008) Iran [40] | |||||||||||||
| Pirdehghan et al. (2016) Iran [25] | - | - | - | - | |||||||||
| Song et al. (2012) China [26] | - | + | + | ||||||||||
| Toko et al. (2016) Kenya [6] | + | + | - | ||||||||||
| Xin et al. (2017) China [36] | |||||||||||||
| Study | Selection Bias | Study Design | Cofounders | Blinding | Data Collection Method | Withdrawals and Dropouts | Global Rating |
|---|---|---|---|---|---|---|---|
| Ajmani et al. (2016) India [24] | 3 | 3 | 3 | 3 | 1 | 3 | Weak |
| Ates et al. (2016) Turkey [37] | 1 | 3 | 3 | 3 | 1 | 1 | Weak |
| Aydogmus et al. (2015) Turkey [38] | 2 | 3 | 3 | 3 | 1 | 1 | Weak |
| Chen et al. (2015) China [35] | 1 | 3 | 1 | 3 | 1 | 1 | Weak |
| Farrant et al. (2009) India [34] | 2 | 3 | 3 | 3 | 1 | 2 | Weak |
| Gbadegesin et al. (2016) Nigeria [27] | 3 | 3 | 3 | 3 | 1 | 3 | Weak |
| Gur et al. (2014) Turkey [41] | 3 | 3 | 3 | 2 | 1 | 1 | Weak |
| Hossain et al. (2010) Pakistan [39] | 3 | 3 | 3 | 3 | 1 | 3 | Weak |
| Maghbooli et al. (2008) Iran [40] | 2 | 3 | 3 | 3 | 1 | 3 | Weak |
| Pirdehghan et al. (2016) Iran [25] | 3 | 3 | 3 | 2 | 1 | 3 | Weak |
| Song et al. (2012) China [26] | 3 | 3 | 3 | 3 | 1 | 3 | Weak |
| Toko et al. (2016) Kenya [6] | 3 | 3 | 1 | 3 | 1 | 3 | Weak |
| Xin et al. (2017) China [36] | 2 | 3 | 1 | 3 | 1 | 1 | Weak |
| Quality Rating | |||
|---|---|---|---|
| Quality Component | Strong (n) | Moderate (n) | Weak (n) |
| Selection bias | 2/13 | 4/13 | 7/13 |
| Study design | 0/13 | 0/13 | 13/13 |
| Confounders | 3/13 | 0/13 | 10/13 |
| Blinding | 0/13 | 2/13 | 11/13 |
| Data collection methods | 13/13 | 0/13 | 0/13 |
| Withdrawal and dropout | 5/13 | 1/13 | 7/13 |
| Global rating | 0/13 | 0/13 | 13/13 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Pligt, P.; Willcox, J.; Szymlek-Gay, E.A.; Murray, E.; Worsley, A.; Daly, R.M. Associations of Maternal Vitamin D Deficiency with Pregnancy and Neonatal Complications in Developing Countries: A Systematic Review. Nutrients 2018, 10, 640. https://doi.org/10.3390/nu10050640
Van der Pligt P, Willcox J, Szymlek-Gay EA, Murray E, Worsley A, Daly RM. Associations of Maternal Vitamin D Deficiency with Pregnancy and Neonatal Complications in Developing Countries: A Systematic Review. Nutrients. 2018; 10(5):640. https://doi.org/10.3390/nu10050640
Chicago/Turabian StyleVan der Pligt, Paige, Jane Willcox, Ewa A. Szymlek-Gay, Emily Murray, Anthony Worsley, and Robin M. Daly. 2018. "Associations of Maternal Vitamin D Deficiency with Pregnancy and Neonatal Complications in Developing Countries: A Systematic Review" Nutrients 10, no. 5: 640. https://doi.org/10.3390/nu10050640