What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Risk of Bias Assessment
2.4. Data Synthesis and Analysis
3. Results
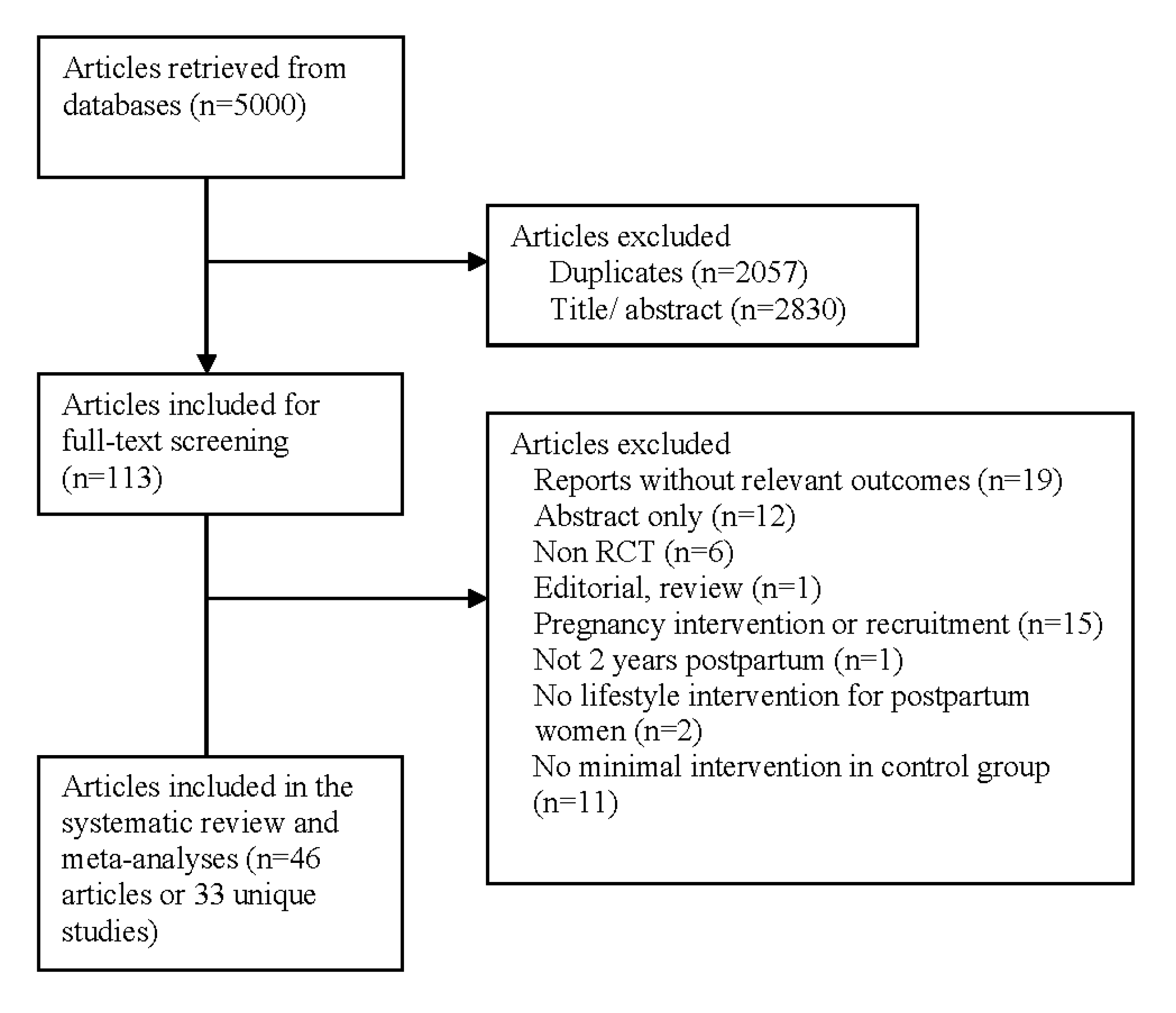
3.1. Identification of Studies
3.2. Study Characteristics
3.3. Participants
3.4. Risk of Bias Assessment
3.5. Meta-Analysis of the Effect of Lifestyle Intervention on Postpartum Women
3.6. Meta-Regression of Behavioural Strategies
3.6.1. Effect of Total Number of Behavioural Strategies
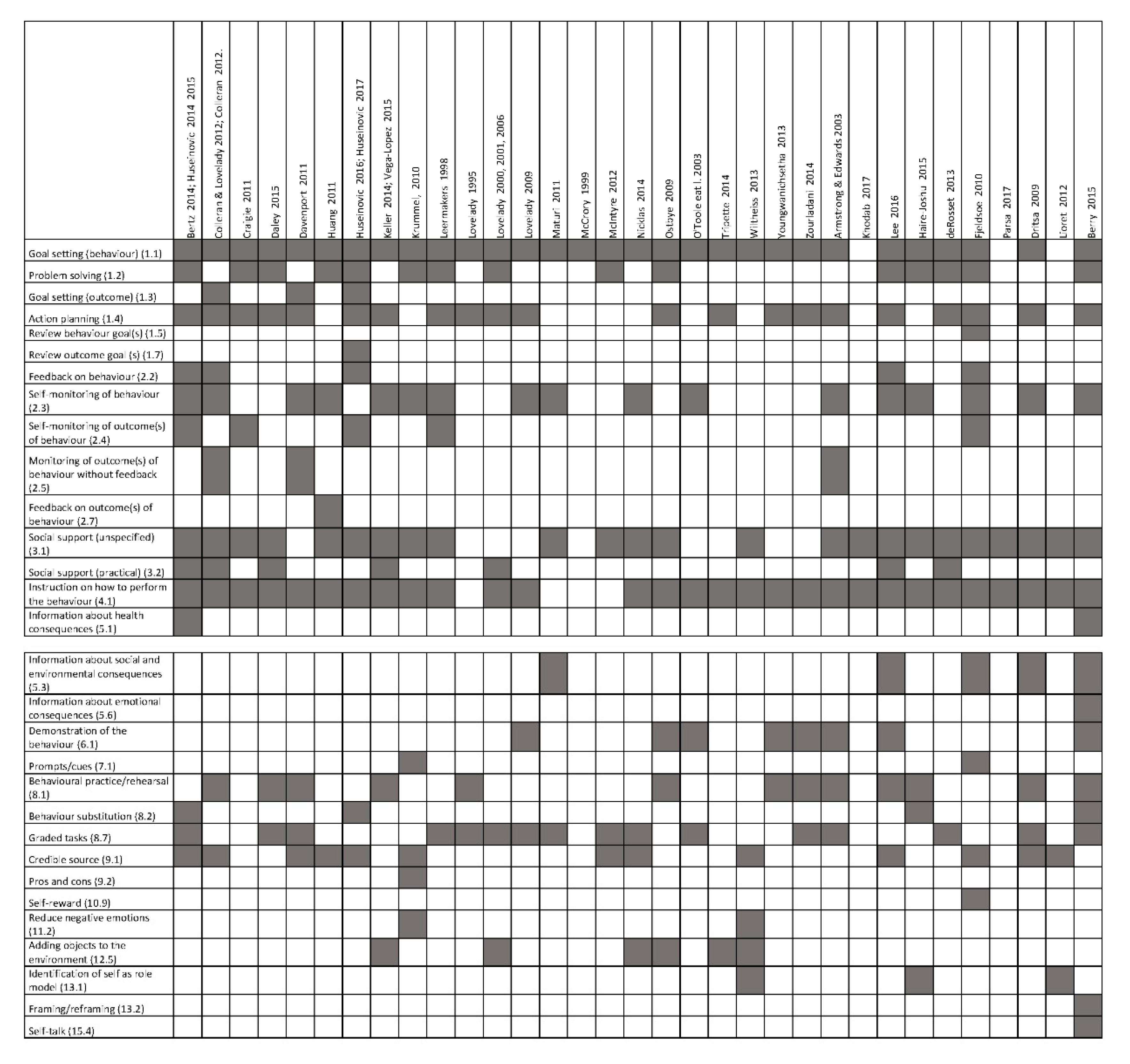
3.6.2. Effect of Individual Behavioural Strategies
3.6.3. Effect of Behavioural Strategies Congruent to Control Theory
4. Discussion
4.1. Principal Findings
4.2. Interpretation of Findings
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Althuizen, E.; van Poppel, M.N.; de Vries, J.H.; Seidell, J.C.; van Mechelen, W. Postpartum behaviour as predictor of weight change from before pregnancy to one year postpartum. BMC Public Health 2011, 11, 165. [Google Scholar] [CrossRef] [Green Version]
- Boghossian, N.S.; Yeung, E.H.; Lipsky, L.M.; Poon, A.K.; Albert, P.S. Dietary patterns in association with postpartum weight retention. Am. J. Clin. Nutr. 2013, 97, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Endres, L.K.; Straub, H.; McKinney, C.; Plunkett, B.; Minkovitz, C.S.; Schetter, C.D.; Ramey, S.; Wang, C.; Hobel, C.; Raju, T.; et al. Postpartum weight retention risk factors and relationship to obesity at 1 year. Obstet. Gynecol. 2015, 125, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Olson, C.M.; Strawderman, M.S.; Hinton, P.S.; Pearson, T.A. Gestational weight gain and postpartum behaviors associated with weight change from early pregnancy to 1 y postpartum. Int. J. Obes. 2003, 27, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villamor, E.; Cnattingius, S. Interpregnancy weight change and risk of adverse pregnancy outcomes: A population-based study. Lancet 2006, 368, 1164–1170. [Google Scholar] [CrossRef]
- Rooney, B.L.; Schauberger, C.W.; Mathiason, M.A. Impact of perinatal weight change on long-term obesity and obesity-related illnesses. Obstet. Gynecol. 2005, 106, 1349–1356. [Google Scholar] [CrossRef]
- Linne, Y.; Dye, L.; Barkeling, B.; Rossner, S. Weight development over time in parous women—The spawn study-15 years follow-up. Int. J. Obes. 2003, 27, 1516–1522. [Google Scholar] [CrossRef] [Green Version]
- Linne, Y.; Barkeling, B.; Rossner, S. Natural course of gestational diabetes mellitus: Long term follow up of women in the spawn study. BJOG 2002, 109, 1227–1231. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Liang, X.; Hill, B.; Teede, H.; Moran, L.J.; O’Reilly, S. A systematic review and meta-analysis of intervention characteristics in postpartum weight management using the tidier framework: A summary of evidence to implementation. Obes. Rev. 2019, 20, 1045–1056. [Google Scholar] [CrossRef]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dombrowski, S.U.; Sneihotta, F.F.; Avenell, A.; Johnston, M.; MacLennan, G.; Araujo-Soares, V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychol. Rev. 2012, 6, 7–32. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.L.; French, D.P. What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behavior-and are they the same? Health Educ. Res. 2011, 26, 308–322. [Google Scholar] [CrossRef] [PubMed]
- Golley, R.K.; Hendrie, G.A.; Slater, A.; Corsini, N. Interventions that involve parents to improve children’s weight-related nutrition intake and activity patterns—What nutrition and activity targets and behaviour change techniques are associated with intervention effectiveness? Obes. Rev. 2011, 12, 114–130. [Google Scholar] [CrossRef]
- Lara, J.; Evans, E.H.; O’Brien, N.; Moynihan, P.J.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Sniehotta, F.F.; White, M.; Mathers, J.C. Association of behaviour change techniques with effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014, 12, 177. [Google Scholar] [CrossRef] [Green Version]
- Nicklas, J.M.; Zera, C.A.; Seely, E.W.; Abdul-Rahim, Z.S.; Rudloff, N.D.; Levkoff, S.E. Identifying postpartum intervention approaches to prevent type 2 diabetes in women with a history of gestational diabetes. BMC Pregnancy Childbirth 2011, 11, 23. [Google Scholar] [CrossRef] [Green Version]
- Carter-Edwards, L.; Ostbye, T.; Bastian, L.A.; Yarnall, K.S.; Krause, K.M.; Simmons, T.J. Barriers to adopting a healthy lifestyle: Insight from postpartum women. BMC Res. Notes 2009, 2, 161. [Google Scholar] [CrossRef] [Green Version]
- Dasgupta, K.; Da Costa, D.; Pillay, S.; De Civita, M.; Gougeon, R.; Leong, A.; Bacon, S.; Stotland, S.; Chetty, V.T.; Garfield, N.; et al. Strategies to optimize participation in diabetes prevention programs following gestational diabetes: A focus group study. PLoS ONE 2013, 8, e67878. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Agosti, M.; MeNu, G. Nutrition in the first 1000 days: Ten practices to minimize obesity emerging from published science. Int. J. Environ. Res. Public Health 2017, 14, 1491. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: a revised tool for assessing risk of bias in randomized trials. BMJ. 2019, 366, 14898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis in R: A Hands-on Guide; 2019. Available online: https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/ (accessed on 15 January 2020).
- deRosset, L.; Berry, D.C.; Sanchez-Lugo, L.; Ritter, K.; Purdum, C.; Santolim, V.; Gilliland, R.; Pender, L. Mama sana... Usted sana: Lessons learned from a postpartum weight loss intervention for hispanic women with infants six months or less. Hisp. Health Care Int. 2013, 11, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Campbell, K.J.; Crawford, D.; Spence, A.C.; Hesketh, K.; McNaughton, S.A. A parent focused child obesity prevention intervention improves some mother obesity risk behaviors: The melbourne infant program. Int. J. Behave. Nutr. Phys. Act. 2012, 9, 100. [Google Scholar] [CrossRef] [Green Version]
- Haire-Joshu, D.L.; Schwarz, C.D.; Peskoe, S.B.; Budd, E.L.; Brownson, R.C.; Joshu, C.E. A group randomized controlled trial integrating obesity prevention and control for postpartum adolescents in a home visiting program. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 88. [Google Scholar] [CrossRef] [Green Version]
- McCrory, M.A.; Nommsen-Rivers, L.A.; Mole, P.A.; Lonnerdal, B.; Dewey, K.G. Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance. Am. J. Clin. Nutr. 1999, 69, 959–967. [Google Scholar] [CrossRef]
- Lovelady, C.A.; Bopp, M.J.; Colleran, H.L.; Mackie, H.K.; Wideman, L. Effect of exercise training on loss of bone mineral density during lactation. Med. Sci. Sports Exerc. 2009, 41, 1902–1907. [Google Scholar] [CrossRef] [Green Version]
- Khodabandeh, F.; Mirghafourvand, M.; KamaliFard, M.; Mohammad-Alizadeh-Charandabi, S.; Jafarabadi, M.A. Effect of educational package on lifestyle of primiparous mothers during postpartum period: A randomized controlled clinical trial. Health Educ. Res. 2017, 32, 399–411. [Google Scholar] [CrossRef] [Green Version]
- Parsa, P.; Alafchi, N.; Soltani, F.; Roshanaei, G. Effects of group counselling on health-promoting behaviours in mothers during postpartum period: A randomised controlled trial. J. Clin. Diagn. Res. 2017, 11, QC09–QC13. [Google Scholar] [CrossRef]
- Zourladani, A.; Zafrakas, M.; Chatzigiannis, B.; Papasozomenou, P.; Vavilis, D.; Matziari, C. The effect of physical exercise on postpartum fitness, hormone and lipid levels: A randomized controlled trial in primiparous, lactating women. Arch. Gynecol. Obstet. 2014, 291, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Youngwanichsetha, S.; Phumdoung, S.; Ingkathawornwong, T. The effects of tai chi qigong exercise on plasma glucose levels and health status of postpartum thai women with type 2 diabetes. Focus Altern. Complement. Ther. 2013, 18, 182–187. [Google Scholar] [CrossRef]
- Nicklas, J.M.; Zera, C.A.; England, L.J.; Rosner, B.A.; Horton, E.; Levkoff, S.E.; Seely, E.W. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: A randomized controlled trial. Obstet. Gynecol. 2014, 124, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leermakers, E.A.; Anglin, K.; Wing, R.R. Reducing postpartum weight retention through a correspondence intervention. Int. J. Obes. 1998, 22, 1103–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostbye, T.; Krause, K.M.; Lovelady, C.A.; Morey, M.C.; Bastian, L.A.; Peterson, B.L.; Swamy, G.K.; Brouwer, R.J.N.; McBride, C.M. Active mothers postpartum. A randomized controlled weight-loss intervention trial. Am. J. Prev. Med. 2009, 37, 173–180. [Google Scholar]
- Fjeldsoe, B.S.; Miller, Y.D.; Marshall, A.L. Mobilemums: A randomized controlled trial of an sms-based physical activity intervention. Ann. Behav. Med. 2010, 39, 101–111. [Google Scholar] [CrossRef]
- Krummel, D.; Semmens, E.; MacBride, A.M.; Fisher, B. Lessons learned from the mothers’ overweight management study in 4 west virginia wic offices. J. Nutr. Educ. Behav. 2010, 42, S52–S58. [Google Scholar] [CrossRef] [Green Version]
- Tripette, J.; Haruka, M.; Yuko, G.; Ryoko, K.; Azusa, S.; Satoshi, H.; Aiko, H.; Motohiko, M. Home-based active video games to promote weight loss during the postpartum period. Med. Sci. Sports Exerc. 2014, 46, 472–478. [Google Scholar] [CrossRef]
- Daley, A.J.; Blamey, R.V.; Jolly, K.; Roalfe, A.K.; Turner, K.M.; Coleman, S.; McGuinness, M.; Jones, I.; Sharp, D.J.; MacArthur, C. A pragmatic randomized controlled trial to evaluate the effectiveness of a facilitated exercise intervention as a treatment for postnatal depression: The pam-pers trial. Psychol. Med. 2015, 45, 2413–2425. [Google Scholar] [CrossRef] [Green Version]
- Huseinovic, E.; Bertz, F.; Brekke, H.K.; Winkvist, A. Two-year follow-up of a postpartum weight loss intervention: Results from a randomized controlled trial. Matern. Child Nutr. 2018, 14, e12539. [Google Scholar] [CrossRef]
- Huseinovic, E.; Bertz, F.; Leu Agelii, M.; Hellebo Johansson, E.; Winkvist, A.; Brekke, H.K. Effectiveness of a weight loss intervention in postpartum women: Results from a randomized controlled trial in primary health care. Am. J. Clin. Nutr. 2016, 104, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernot, J.; Lewis, L.; Olds, T.; Maher, C. Effectiveness of a facebook-delivered physical activity intervention for postpartum women: A randomized controlled trial. J. Phys. Act. Health 2019, 16, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Keller, C.; Ainsworth, B.; Records, K.; Todd, M.; Belyea, M.; Vega-Lopez, S.; Permana, P.; Coonrod, D.; Nagle-Williams, A. A comparison of a social support physical activity intervention in weight management among post-partum latinas. BMC Public Health 2014, 14, 971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovelady, C.A.; Garner, K.E.; Moreno, K.L.; Williams, J.P. The effect of weight loss in overweight, lactating women on the growth of their infants. N. Engl. J. Med. 2000, 342, 449–453. [Google Scholar] [CrossRef]
- Lovelady, C.A.; Stephenson, K.G.; Kuppler, K.M.; Williams, J.P. The effects of dieting on food and nutrient intake of lactating women. J. Am. Diet. Assoc. 2006, 106, 908–912. [Google Scholar] [CrossRef]
- Lovelady, C.A.; Williams, J.P.; Garner, K.E.; Moreno, K.L.; Taylor, M.L.; Leklem, J.E. Effect of energy restriction and exercise on vitamin b-6 status of women during lactation. Med. Sci. Sports Exerc. 2001, 33, 512–518. [Google Scholar] [CrossRef]
- Zilberman-Kravits, D.; Meyerstein, N.; Abu-Rabia, Y.; Wiznitzer, A.; Harman-Boehm, I. The impact of a cultural lifestyle intervention on metabolic parameters after gestational diabetes mellitus a randomized controlled trial. Matern. Child Health J. 2018, 22, 803–811. [Google Scholar] [CrossRef]
- Presseau, J.; Ivers, N.M.; Newham, J.J.; Knittle, K.; Danko, K.J.; Grimshaw, J.M. Using a behaviour change techniques taxonomy to identify active ingredients within trials of implementation interventions for diabetes care. Implement. Sci. 2015, 10, 55. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Dunbar, J.A.; Versace, V.L.; Janus, E.; Wildey, C.; Skinner, T.; O’Reilly, S. Comparing a telephone- and a group-delivered diabetes prevention program: Characteristics of engaged and non-engaged postpartum mothers with a history of gestational diabetes. Diabetes Res. Clin. Pract. 2017, 126, 254–262. [Google Scholar] [CrossRef]
- Smith, D.M.; Taylor, W.; Lavender, T. Behaviour change techniques to change the postnatal eating and physical activity behaviours of women who are obese: A qualitative study. BJOG 2016, 123, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Rutten, G.M.; Meis, J.J.; Hendriks, M.R.; Hamers, F.J.; Veenhof, C.; Kremers, S.P. The contribution of lifestyle coaching of overweight patients in primary care to more autonomous motivation for physical activity and healthy dietary behaviour: Results of a longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 86. [Google Scholar] [CrossRef] [Green Version]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Association of changes in diet quality with total and cause-specific mortality. N. Engl. J. Med. 2017, 377, 143–153. [Google Scholar] [CrossRef]
- Adamson, L.; Brown, W.; Byles, J.; Chojenta, C.; Dobson, A.; Fitzgerald, D.; Hockey, R.; Loxton, D.; Powers, J.; Spallek, M.; et al. Women’s Weight: Findings from the Australian Longitudinal Study on Women’s Health: Report Prepared for the Australian Government Department of Health and Ageing; 2007. Available online: https://www.alswh.org.au/images/content/pdf/major_reports/2007_major_report_b.pdf (accessed on 15 January 2020).
- Zheng, Y.; Manson, J.E.; Yuan, C.; Liang, M.H.; Grodstein, F.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA 2017, 318, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Dusseldorp, E.; van Genugten, L.; van Buuren, S.; Verheijden, M.W.; van Empelen, P. Combinations of techniques that effectively change health behavior: Evidence from meta-cart analysis. Health Psychol. 2014, 33, 1530–1540. [Google Scholar] [CrossRef] [PubMed]
- Gillison, F.B.; Rouse, P.; Standage, M.; Sebire, S.J.; Ryan, R.M. A meta-analysis of techniques to promote motivation for health behaviour change from a self-determination theory perspective. Health Psychol. Rev. 2019, 13, 110–130. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Country | Sample Size | Intervention | Active Phase (week) | Risk Factor at Inclusion | Outcomes |
|---|---|---|---|---|---|---|
| Berry, 2015 | USA | 60 | Diet and exercise | 6 months | Baseline BMI ≥25 kg/m2 | Physical activity |
| Bertz, 2015 | Sweden | 68 | Diet and exercise | 12 weeks | Prepregnancy 25–35 kg/m2 | Weight, energy intake, physical activity |
| Colleran, 2012 | USA | 31 | Diet and exercise | 16 weeks | Baseline BMI 25–30 kg/m2 | Weight, energy intake, physical activity |
| Craigie, 2011 | UK | 52 | Diet and exercise | 12 weeks | Baseline BMI ≥25 kg/m2 | Weight, physical activity |
| Daley, 2015 | UK | 94 | Exercise | 6 months | Postnatal depression | Weight |
| Davenport, 2011 | Canada | 47 | Diet and exercise | 16 weeks | Baseline BMI ≥25 kg/m2 or retained ≥5 kg from pregnancy | Weight, energy intake |
| deRosset, 2013 | USA | 24 | Diet and exercise | 12 weeks | Prepregnancy BMI ≥25 kg/m2 | Physical activity |
| Dritsa, 2009 | Canada | 88 | Exercise | 12 weeks | Postnatal depression | Physical activity |
| Fjeldsoe, 2010 | Australia | 88 | Exercise | 12 weeks | - | Physical activity |
| Holmes, 2018 | Northern Ireland | 60 | Diet and exercise | 6 months | Prepregnancy or baseline BMI ≥25 kg/m2, gestational diabetes | Weight |
| Huang, 2009 | Taiwan | 240 | Diet and exercise | 6 months | - | Weight |
| Huseinovic, 2016 | Sweden | 110 | Diet | 12 weeks | Baseline BMI ≥27 kg/m2 | Weight, energy intake, physical activity |
| Keller, 2014 | USA | 139 | Exercise | 12 months | Baseline BMI 25–35 kg/m2 | Weight, energy intake, physical activity |
| Kernot, 2019 | Australia | 120 | Exercise | 6 weeks | - | Physical activity |
| Khodabandeh, 2017 | Iran | 220 | Diet and exercise | 6 weeks | - | Physical activity |
| Krummel, 2010 | USA | 151 | Diet and exercise | 12 months | - | Weight, physical activity |
| Leermakers,1998 | USA | 90 | Diet and exercise | 6 months | Baseline BMI ≥22 kg/m2 and retained ≥6.8 kg from pregnancy | Weight |
| Lioret, 2012 | Australia | 542 | Diet and exercise | 15 months | - | Physical activity |
| Lovelady, 2000 | USA | 48 | Diet and exercise | 12 weeks | Baseline BMI 25–30 kg/m2 | Weight, energy intake, physical activity |
| Lovelady, 1995 | USA | 38 | Exercise | 10 weeks | - | Weight, energy intake, physical activity |
| Lovelady, 2009 | USA | 24 | Exercise | 16 weeks | Baseline BMI 20–30 kg/m2 | Weight, energy intake, physical activity |
| Maturi, 2011 | Iran | 70 | Exercise | 12 weeks | - | Weight, physical activity |
| McCrory,1999 | USA | 68 | Diet and exercise | 11 days | - | Weight, physical activity |
| McIntyre, 2012 | Australia | 28 | Exercise | 12 weeks | Gestational diabetes | Weight |
| Nicklas, 2014 | USA | 75 | Diet and exercise | 12 months | Gestational diabetes | Weight |
| Ostbye, 2009 | USA | 450 | Diet and exercise | 9 months | Prepregnancy BMI ≥25 kg/m2 | Weight, energy intake, physical activity |
| O’Toole, 2003 | USA | 40 | Diet and exercise | 12 weeks | Prepregnancy BMI 25–29.9 kg/m2 | Weight, energy intake, physical activity |
| Parsa, 2017 | Iran | 120 | Diet and exercise | 3 weeks | - | Physical activity |
| Tripette, 2014 | Japan | 34 | Exercise | 40 days | Baseline BMI >22 kg/m2 | Weight, energy intake, physical activity |
| Wiltheiss, 2012 | USA | 400 | Diet and exercise | 8 months | Prepregnancy and baseline BMI ≥25 kg/m2 | Weight, energy intake |
| Youngwanichsetha, 2013 | Thailand | 69 | Exercise | 12 weeks | Type 2 diabetes | Weight |
| Zilberman, 2018 | Israel | 180 | Diet and exercise | 24 months | Gestational diabetes | Weight, physical activity |
| Zourladani, 2015 | Greece | 42 | Exercise | 12 weeks | - | Weight, physical activity |
| Behavioural Strategies | β | 95% Confidence Interval | P-Value | Adjusted R-Squared (%) |
|---|---|---|---|---|
| Total number of behavioural strategies | −0.36 | −0.65, −0.07 | 0.02 | 49.40 |
| Behavioural strategies consistent with control theory | −0.56 | −1.12, −0.20 | 0.01 | 62.15 |
| 1.2 Problem solving | −1.74 | −3.43, −0.05 | 0.05 | 32.33 |
| 1.3 Goal setting (outcome) | −1.91 | −3.78, −0.04 | 0.05 | 39.72 |
| 1.4 Action planning | −0.69 | −3.14, 1.77 | 0.55 | 0.00 |
| 1.7 Reviewing outcome goal | −3.94 | −6.51, −1.36 | 0.01 | 72.05 |
| 2.2 Feedback on behaviour | −2.81 | −4.26, −1.37 | 0.00 | 87.59 |
| 2.3 Self-monitoring of behaviour | 0.44 | −1.51, 2.38 | 0.63 | 0.00 |
| 2.4 Self-monitoring of outcome of behaviour | −3.20 | −5.06, −1.33 | 0.00 | 80.22 |
| 2.5 Monitoring of outcome of behaviour without feedback | −0.57 | −3.23, 2.10 | 0.65 | 0.00 |
| 3.1 Social support (unspecified) | −1.21 | −2.97, 0.55 | 0.16 | 9.49 |
| 3.2 Social support (practical) | −0.75 | −2.81, 1.31 | 0.44 | 0.00 |
| 4.1 Instructions on how to perform the behaviour | 0.45 | −1.52, 2.48 | 0.62 | 0.00 |
| 5.1 Information about health consequences | −1.71 | −5.44, 2.01 | 0.33 | 2.61 |
| 6.1 Demonstration of the behaviour | 1.22 | −0.80, 3.25 | 0.21 | 5.91 |
| 8.1 Behavioural practice/rehearsal | 0.87 | −1.01, 2.76 | 0.33 | 0.00 |
| 8.2 Behaviour substitution | −3.20 | −5.06, −1.33 | 0.00 | 80.22 |
| 8.7 Graded tasks | 0.84 | −1.03, 2.71 | 0.34 | 0.00 |
| 9.1 Credible source | −1.73 | −3.28, −0.17 | 0.03 | 38.81 |
| 11.2 Reduce negative emotions | 0.31 | −3.06, 3.68 | 0.84 | 0.00 |
| 12.5 Adding objects to the environment | 0.40 | −1.57, 2.36 | 0.66 | 0.00 |
| 13.1 Identification of self as a role model | 0.31 | −3.06, 3.68 | 0.84 | 0.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.; Hill, B.; Pirotta, S.; O’Reilly, S.; Moran, L. What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 237. https://doi.org/10.3390/jcm9010237
Lim S, Hill B, Pirotta S, O’Reilly S, Moran L. What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(1):237. https://doi.org/10.3390/jcm9010237
Chicago/Turabian StyleLim, Siew, Briony Hill, Stephanie Pirotta, Sharleen O’Reilly, and Lisa Moran. 2020. "What Are the Most Effective Behavioural Strategies in Changing Postpartum Women’s Physical Activity and Healthy Eating Behaviours? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 1: 237. https://doi.org/10.3390/jcm9010237