Pterins as Diagnostic Markers of Mechanical and Impact-Induced Trauma: A Systematic Review


1
Institution for Physical Activity and Nutrition (IPAN), School of Exercise and Nutrition Sciences, Deakin University, Geelong, VIC 3220, Australia
2
School of Biological Sciences, University of Canterbury, Christchurch 8140, New Zealand
3
Department of Radiology, University of Otago Christchurch, P.O. Box 4345, Christchurch 8011, New Zealand
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2019, 8(9), 1383; https://doi.org/10.3390/jcm8091383
Submission received: 16 July 2019
/
Revised: 21 August 2019
/
Accepted: 27 August 2019
/
Published: 3 September 2019
(This article belongs to the Section Epidemiology & Public Health)
Abstract
:We performed a systematic review of the literature to evaluate pterins as biomarkers of mechanical and impact-induced trauma. MEDLINE and Scopus were searched in March 2019. We included in vivo human studies that measured a pterin in response to mechanical or impact-induced trauma with no underlying prior disease or complication. We included 40 studies with a total of 3829 subjects. Seventy-seven percent of studies measured a significant increase in a pterin, primarily neopterin or total neopterin (neopterin + 7,8-dihydroneopterin). Fifty-one percent of studies measured an increase within 24 h of trauma, while 46% measured increases beyond 48 h. Pterins also showed promise as predictors of post-trauma complications such as sepsis, multi-organ failure and mortality. Exercise-induced trauma and traumatic brain injury caused an immediate increase in neopterin or total neopterin, while patients of multiple trauma had elevated pterin levels that remained above baseline for several days. Pterin concentration changes in response to surgery were variable with patients undergoing cardiac surgery having immediate and sustained pterin increases, while gastrectomy, liver resection or hysterectomy showed no change. This review provides systematic evidence that pterins, in particular neopterin and total neopterin, increase in response to multiple forms of mechanical or impact-induced trauma.
Keywords:
biopterin; exercise; neopterin; surgery; tetrahydrobiopterin; trauma; traumatic brain injury1. Introduction
Pterins are biologically active bi-cyclic compounds. Pterins have been utilised as biomarkers because of their involvement in inflammation [1], oxidative stress [2] and aromatic amino acid hydroxylation [3] since they were discovered in 1889 [4]. Neopterin and tetrahydrobiopterin (BH4) are examples of pterins used to assess changes in immune system activation and oxidative status, as well as deficiencies in monoamine neurotransmitter synthesis and nitric oxide availability, respectively. Neopterin is the oxidative product of 7,8-dihydroneopterin, a metabolic derivative of guanosine triphosphate (GTP) produced by monocytes and macrophages during γ-interferon (γ-IFN)-stimulated immune activation [5]. Neopterin has been used a useful measure of exercise-induced stress [6], cancer [7], neuromuscular disease [8], human immunodeficiency virus (HIV) [9], sepsis [10] and vascular disease [11]. BH4 is also a product of GTP metabolism and used to diagnose numerous neurological diseases, including phenylketonuria, due to its involvement as a co-factor in many hydroxylase enzyme reactions [12].
Accurate diagnosis and management of mechanical or impact-induced trauma is critical for patient monitoring and treatment. Major mechanical incident can cause immediate structural damage that results in the loss of muscle plasmalemma integrity, organ perforation or bone breaks and a secondary insult of immune cells [13]. Next, a co-ordinated inflammatory and anti-inflammatory response [14] work to remove and remodel damaged tissue while also maintaining homeostasis. In severe cases, infection, systemic inflammatory response syndrome (SIRS), sepsis, multi-organ dysfunction (MOD) and even mortality can occur [15,16,17]. The critical junction between patient admittance and initial treatment can determine the level of morbidity and mortality [18]. Thus, the need for sensitive and accurate diagnostic and prognostic biomarkers of trauma is critical for initial diagnosis, monitoring of patient progress and treatment efficacy.
Pterins are also useful biomarkers of mechanical and impact-induced trauma. Since 1988 [19], studies have utilised the biomarker potential of pterins to accurately assess the extent of initial trauma and the subsequent monitoring of injury progression or recovery. In this systematic review, we sought to gather all published literature measuring pterins in response to mechanical or impact-induced trauma in humans with the purpose of understanding if pterins provide a sensitive and accurate biomarker.
2. Experimental Section
Systematic Review: We performed a thorough systematic search of the research literature for the use of pterins as biomarkers of mechanical and impact-induced trauma. We performed the literature search in MEDLINE and Scopus on 7 March 2019. The search terms were “pterin” OR “dihydropterin” OR “neopterin” OR “dihydroneopterin” OR “biopterin” OR “dihydrobiopterin” OR “tetrahydrobiopterin” OR “dihydroxanthopterin” OR “xanthopterin” OR “isoxanthopterin” OR “sepiapterin” OR “monapterin” OR “oncopterin” OR “leucopterin” AND “muscle damage” OR “trauma” OR “accident” OR “exercise” OR “sport” OR “surgery”. We delimited studies to those in English and involving human subjects.
Study Inclusion and Exclusion Criteria: We considered studies for review that met the following inclusion criteria: (1) a pterin was measured, (2) severe mechanical or impact-induced trauma was evident and (3) the study was conducted on humans. We included exercise that had a significant impact component that resulted in muscle damage, as well as studies that were accidental (car accident) or elective (surgery). We included studies that measured pterins in all media, including urine, plasma, serum, cerebrospinal fluid (CSF), saliva or tissue and did not exclude studies based on design, unless they were systematic or scoping reviews and meta-analyses. Studies meeting the following exclusion criteria were not considered for review: (1) patients undergoing transplant surgery, (2) pterin supplementation studies, (3) surgery where an underlying disease existed unless accompanied by select co-morbidities such as hypertension of diabetes (specified in the surgical table), (4) sepsis unless resulting from trauma, (5) studies on animals, (6) ex vivo pterin analysis of tissue collected from patients following trauma or (7) burn injuries. Finally, there were no exclusion criteria for race, ethnicity, age, sex, nationality, socioeconomic status or education level of the subjects. After the initial systematic review, all authors appropriately screened the articles and disagreements were resolved through discussion. A meta-analysis was not completed because reporting of absolute pterin concentrations were sparse between studies.
3. Results
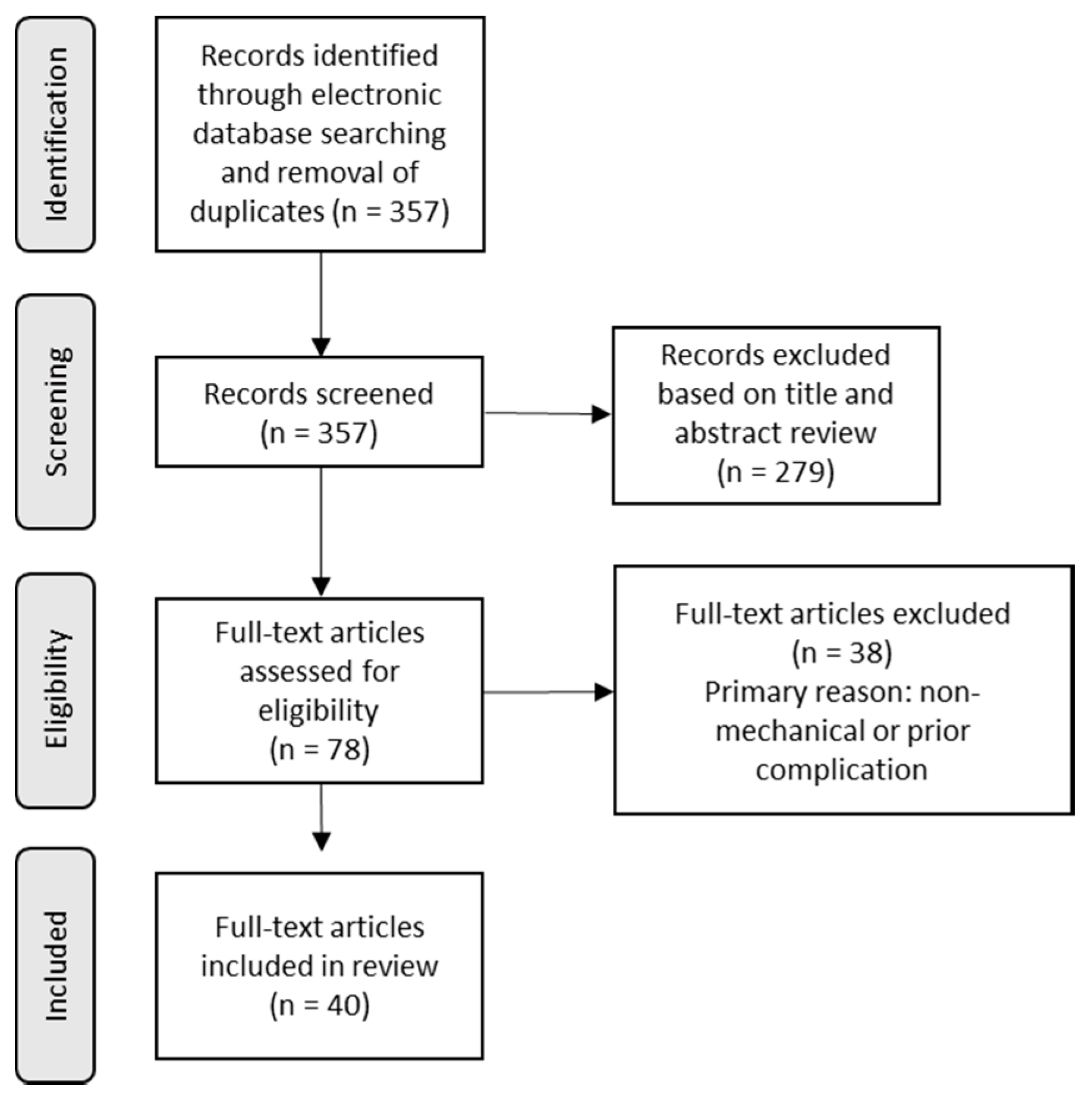
Selection of Studies: We identified 357 publications through the electronic databases search after removal of duplicates. After review of the title and abstract, we excluded 279 articles. We fully evaluated 78 full-text articles. We excluded 37 articles based on the inclusion/exclusion criteria, resulting in 40 total articles for the systematic review (Figure 1). We separated included articles into four categories of mechanical or impact-induced trauma; exercise/sport, surgery, traumatic brain injury (TBI) and multiple injuries (polytrauma). We detailed individual study results in Table 1, Table 2, Table 3 and Table 4, including inclusion/exclusion criteria and the primary outcome of the pterin response. Therefore, we will not present the detailed results of each included study, but rather an overview of the collective findings.
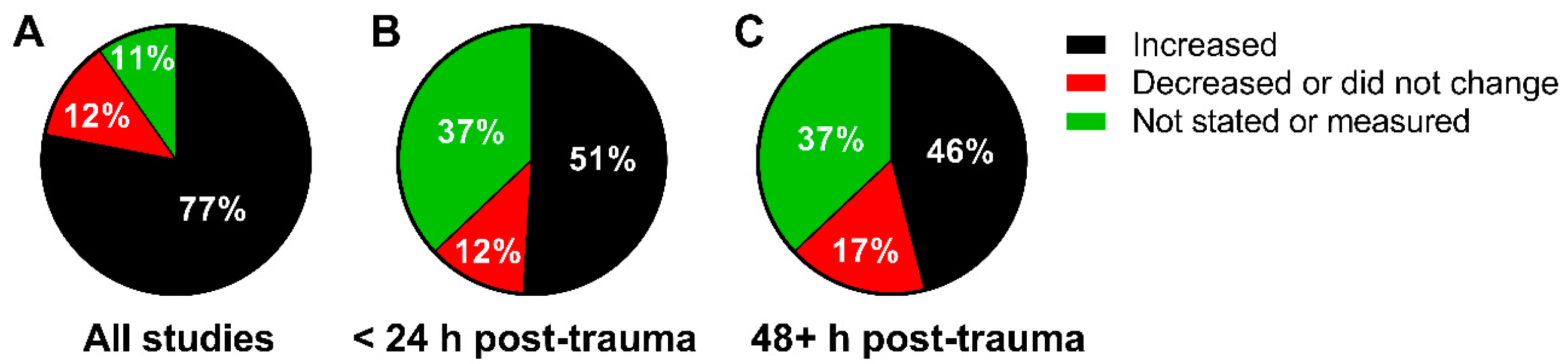
Overall Finding: A total of 3829 subjects from 40 studies have been compiled (Figure 2). Seventy-seven percent of the studies reported an increase in a pterin in response to mechanical or impact-induced trauma (Figure 2A). In the studies that reported a pterin response timeline to trauma, 51% increased within 24 hours (Figure 2B), while 46% remained elevated for greater than 48 hours (Figure 2C).
Exercise Trauma: Nine total articles met the inclusion criteria for exercise-induced trauma (Table 1). Articles were published between 2015–2017, indicating the use of pterins in exercise-induced trauma is relatively novel. All nine articles measured total neopterin (neopterin + 7,8-dihydroneopterin), six measured neopterin and total neopterin and one measured biopterin, total biopterin (biopterin + 7,8-dihydrobiopterin + BH4) and xanthopterin. Each study included elite amateur or professional athletes and measured a change in urinary pterins associated with rugby union or mixed martial arts (MMA), two sports that both endure repeated high-force impacts resulting in muscle damage and inflammation [20]. The evidence indicates a single game of rugby union or an MMA contest or training session causes an immediate increase in all pterins measured. It is noted that an increase in pterins may be specific to the impacts of the sport because neopterin concentrations do not always change in response to exercise devoid of impacts [21]. Changes in neopterin are transient following rugby union, returning to baseline within 24 h of a game while it can remain elevated following an MMA training session up to 24 h post-contest. Interestingly, only a continuous increase in neopterin and total neopterin showed evidence of sustained oxidative stress/inflammation over an extended training camp in MMA (6 weeks), while a whole season of rugby union did not affect concentrations, indicating the intensity and repetition of impact during MMA training may be of a greater intensity than rugby union. Collectively, the data indicates that pterins, in particular neopterin and total neopterin, are sensitive markers of exercise/sport-induced trauma and reflect changes in oxidative stress and inflammation.
Surgery: Fifteen articles met the inclusion criteria for surgery-induced trauma (1988–2019; Table 2). Pterins were measured primarily following cardiac surgery with or without cardiopulmonary bypass, but were also measured following herniotomy, cholecystectomy, rectal or colon surgery, ypsilon graft, liver resection, hernia, vulvectomy or hysterectomy, gastrectomy or knee replacement. All 15 articles measured either neopterin or total neopterin, while only one measured BH4, indicating a preference for a marker of immune system activation. Furthermore, all but one study measured these pterins in either plasma or serum. All but two articles also had specific exclusion criteria to evaluate the change in biomarker concentrations to the surgical procedure, including pterins (detailed in Table 2). One study investigated the change in neopterin in neonates and infants/children, while all other studies recruited adults. Procedures that involved a form of cardiac surgery always resulted in a significant increase in neopterin within 6-hours post-surgery that remained elevated for several days. Neopterin was also higher in those patients that developed post-surgical complications such as sepsis, delirium, cardiac dysfunction or acute kidney injury following surgery. A similar neopterin response was also observed in patients undergoing hernia surgery or knee replacement surgery; however, there were limited changes in neopterin in response to all other surgeries while some patients showed a decrease in concentration post-surgery, likely because of pre-surgical complications associated with immune system activation or interactions with general anaesthesia down-regulating the immune system. Taken together, the evidence indicates neopterin may only increase in response to cardiac surgery and other limited surgical procedures and identify patients at greater risk of post-surgical complications.
Traumatic Brain Injury: Two articles met the inclusion criteria for pterin changes in response to TBI ([44,45]; Table 3). Both articles, published in 2001 and 2002, were by the same group and measured neopterin concentrations in patients in response to an “isolated” or “severe” TBI. Patients presented with a Glasgow Coma Score at admission equal to or less than eight and associated abnormalities of the brain via computer-aided tomography. Neopterin was measured in serum and CSF. In one study, serum neopterin increased in response to the TBI and remained elevated 14 days post-surgery. Neopterin in CSF also increased and remained elevated up to 21 days post-surgery. The second study only presented CSF neopterin concentrations in relation to another biomarker, but some patients had levels > 30 ng/mL. No further studies have measured any pterin in response to TBI since 2002. The limited data available from these two studies does indicate TBI increases plasma neopterin concentrations.
Multiple Injuries (Polytrauma): Sixteen total articles published between 1989 and 2017 met the inclusion criteria for multiple injury-induced trauma on changes in pterins (Table 4). All studies involved severe trauma or hip-fracture and patients were greater than 16 years of age. In severe trauma studies, patients were included based on their injury severity score (≥ 16 to a maximum of 66 in a single case-study) or APACHE (acute physiology, age, chronic health evaluation) score (severity of disease; 18.9). Exclusion criteria, where stated, included patients with an underlying disease, immunosuppressive therapy, immunodeficiences, corticosteroid treatment or in some cases, patients did not survive during the data collection period. All 16 studies measured neopterin with only one measuring total neopterin. No studies measured other pterins. Neopterin and total neopterin were measured in urine, serum, plasma and CSF. In all studies, neopterin and total neopterin significantly increased. Neopterin concentrations remained elevated 2–14 days post-trauma, which corresponded with the final measurement of a study design. Neopterin concentrations, irrespective of the bio-fluid, correlated with the severity of trauma [(ISS (injury severity score) and APACHE score] and were higher in non-surviving patients, patients suffering from organ failure as a result of trauma (one study did not see a relationship), patients with delirium and/or cognitive impairment. Neopterin also continually increases in the days following trauma and is a good predictor of mortality up to one-year post-bone fracture in the elderly. Overall, multiple trauma or bone fracture causes an increase in neopterin concentrations that are associated with clinically relevant outcomes, including death.
4. Discussion
The purpose of this systematic review was to critically evaluate studies that measured pterins in response to mechanical or impact-induced trauma. Only studies measuring a pterin in humans in response to mechanical or impact-induced trauma were considered and it is the first survey to date of pterins as diagnostic and prognostic biomarkers of trauma. Overall, this review provides evidence that pterins increase in response to trauma. However, different effects and changes in pterin concentration were identified when the type of trauma was considered. Collectively, pterins, particularly neopterin and total neopterin, increase after trauma, remain elevated and may be a predictor of several clinically important patient outcomes.
Review of the literature identified 40 articles that measured pterins in response to trauma, all of which measured either neopterin, total neopterin or both. 7,8-Dihydroneopterin is an antioxidant synthesized from γ-IFN-activated monocytes/macrophages during immune system activation and can be oxidized to neopterin. Neopterin’s highly fluorescent properties and easy detection methods [6,61,62] make it a popular candidate to measure an inflammatory response, which may explain why every article considered in this review measured it in reaction to various forms of trauma. However, the use of neopterin and not the simultaneous measurement of 7,8-dihydroneopteirn as a marker of immune system activation has been a topic of discussion. It is suggested that the measurement of neopterin alone might only be an indicator of oxidative stress and thus, does not reflect the true level of inflammation [2,63]. Therefore, the increase in neopterin associated with mechanical or impact-induced trauma might be a reflection of elevated oxidative stress rather than cumulative inflammation. However, the simultaneous increase in neopterin and total neopterin following knee replacement surgery [43], an MMA contest [27,29,30] or rugby game [22] suggests neopterin might reflect immune system activation in response to trauma as well as oxidative stress.
While neopterin was measured in every study, biopterin, BH4 and total biopterin were also measured in response to trauma. BH4 is enzymatically synthesized from GTP and metabolized to dihydrobiopterin while acting as a co-factor for the amino acid hydroxylases and nitric oxide synthases. Dihydrobiopterin is salvaged to BH4 or oxidized to biopterin. Thus, the measurement of biopterins can be indicative of oxidative stress, monoamine neurotransmitter synthesis and nitric oxide availability (nitric oxide-induced vasodilation and other functions [64]). Given the biopterins ability to indicate several acute and chronic biological conditions, and trauma is associated with oxidative stress and blood flow [65,66,67], it was surprising the biopterins have not been measured in abundance. The lack of biopterins as biomarkers may be due to the multitude of processes that produce biopterin, or use BH4 as a co-factor. The only article that clearly states a change in biopterins noted significant increases following four rugby games that was positively associated with the number of impacts a player experienced during the game [28]. Therefore, we suggest, on limited data, that biopterins may provide a general but sensitive biomarker of trauma and should be considered in future studies. Furthermore, xanthopterin was the only other pterin measured, once again in the same study on several rugby games. Xanthopterin, a catabolite of biopterin, was also increased following a rugby game and associated with the number of impacts experienced by a player. Collectively, this evidence and other research showing isoxanthopterin is elevated in muscle degenerative diseases [68], indicates other pterins may be useful indicators of trauma.
Pterins are synthesized from all cell types and tissues. Therefore, measurement of pterins in response to mechanical or impact-induced trauma can be taken in multiple bio-fluids with similar efficacy. While pterin measurements were limited to urine and CSF in exercise and brain injury studies, respectively, pterins were measured almost selectively in plasma or serum in multi-trauma or surgical studies. Blood and CSF media do provide a reliable and direct measurement of pterins in circulation. However, urinary pterins also increase in response to various trauma and it does provide a medium that can be readily accessed for multiple measurements through catheterization or non-invasively using a collection container. Urinary pterins are also able to be measured by HPLC, RIA or ELISA and require less sample clean up prior to measurement; however, urinary pterin concentrations require normalization by creatinine, specific gravity or osmolality to account for changes in hydration. Collectively, pterins increase in all bio-fluids following mechanical or impact-induced trauma, but for longitudinal analyses that require follow-up measurements, urine may be a suitable media.
Exercise Trauma: Studies on exercise-induced trauma, typically those associated with repeated high-force impacts like rugby or MMA, have utilized biomarkers like creatine kinase [69], myoglobin [70] or C-reactive protein [71] to measure changes in muscle damage and inflammation. The results of this review provide evidence that repeated high-force impacts in rugby union or MMA always result in a transient increase in several pterins and that this increase is mostly associated with the number of total impacts experienced by a competitor. Furthermore, the studies that collected samples at multiple time-points following exercise noted that neopterin or total neopterin was sustained for up to 24 hours, indicating they can be used to monitor post-traumatic changes in immune system activation following impact-induced trauma [30]. Two studies further defined the potential of total neopterin to measure the longitudinal response to repetitive insult, which might mimic a multiple-trauma patient undergoing repeated surgical intervention and long hospital stays. During a 20-week rugby season, where players complete several training sessions (fitness and weight-lifting) and a competitive game on a weekly basis, total neopterin levels did not change [25]. However, during a six-week MMA training camp where athletes complete weight-lifting and several contact sessions/week, neopterin and total neopterin steadily increased throughout the duration [29]. When assessing exercise-induced trauma using pterins, the evidence suggests pterins should be immediately quantified to understand the acute stress, while weekly monitoring may provide important information about adaptation to repeated insults or development of over-training. Overall, the evidence indicates neopterin and total neopterin are sensitive biomarkers of impact-induced trauma in sport and exercise.
Surgery: Surgical intervention is highly invasive and initiates a cascade of inflammatory processes [72]. The results of this review indicate neopterin and/or total neopterin increase with selective surgeries. Therefore, neopterin and/or total neopterin is a useful diagnostic and prognostic marker of surgical intervention. Interestingly, the pterins were only responsive to selective surgeries, which suggests they may only be useful under specific circumstances. For example, any thoracic surgery, with or without cardiopulmonary bypass, always resulted in an increase [35], which likely reflects the level of trauma inflicted on the patient to access the heart. It would be interesting to compare neopterin levels following cardiac key hole surgery. Surgeries such as hysterectomy [39] or gastrectomy [42] did not affect neopterin concentrations, suggesting there is a much lower level of trauma involved in these particular procedures. Differentiating between the level of stress associated with each surgical procedure is difficult but the rise in neopterin is not thoracic-specific, with knee replacement surgery [43] also resulting in an increase. There is also evidence that neopterin remains elevated for several days post-surgery [37] and is higher in patients that develop sepsis [31] and become delirious [38]. Therefore, in a clinical setting, the pre to post change in pterins could provide an assessment of acute surgical stress while long-term daily monitoring of pterins might be advantageous for selective patients that develop post-surgical complications. Because neopterin and total neopterin are considered reliable and sensitive markers of oxidative stress and inflammation, clinicians should consider daily measurements until concentrations either return to “normal” values or remain steady below pre-surgical levels for several days. These data suggest neopterin can provide indicative data on the acute and chronic response to selective surgical interventions, especially where post-operative infection complications are suspected.
Traumatic Brain Injury: Traumatic brain injury is associated with inflammation [73] and oxidative stress [74]. While limited studies have measured any pterin in response to TBI, two studies which have noted a significant increase in neopterin also reported a sustained elevation for 14–21 days post-surgery [44,45]. Whether the increase in neopterin is a measure of oxidative stress or inflammation is unknown but it provides evidence that neopterin may be a sensitive marker of TBI. However, because surgery followed the TBI, the surgical intervention could have an effect on neopterin concentrations. It is also interesting that no further studies have explored the use of neopterin or any other pterin in response to TBI given the sensitivity of the two published studies. While numerous studies are exploring biomarkers of TBI [75], perhaps the inclusion of neopterin and/or total neopterin may provide some added diagnostic and prognostic benefit. Therefore, in cases of TBI that arise from sport, accidents or work-related injuries, neopterin and/or total neopterin should be measured at patient admittance and daily until values return to “normal”.
Multiple Trauma (Polytrauma): Multiple trauma always results in an acute and chronic increase in neopterin and total neopterin, the latter only being measured in one study [59]. The sensitivity of neopterin in response to multiple trauma seems greatest compared to the three other categories of this review. Neopterin concentrations, whether in the urine, plasma, blood or CSF, significantly increase, but because 15 of the 16 studies only measured neopterin and not total neopterin, the full scope of neopterin’s diagnostic and prognostic capability is unclear. Nonetheless, it is evident that multiple trauma [54] or a bone fracture [60] results in a sustained increase in neopterin. Most importantly, it is the association of neopterin with clinically relevant outcomes like organ failure [50], survival [49] and the severity of the trauma [53] that indicate neopterin is a strong biomarker candidate for identifying the degree of multiple trauma and the likelihood of developing post-trauma complications. Therefore, in cases where patients experience multi-trauma, the evidence suggests neopterin and/or total neopterin should be immediately assessed to quantify the extent of injury and then repeatedly measured every 12–24 hours to monitor development of other complications. Because neopterin was always greater in non-surviving patients, it may provide sensitive and reliable information to clinicians regarding an appropriate course of treatment.
Limitations: There are limitations to this systematic review: (1) the number of studies measuring a pterin following traumatic brain injury is severely limited. It is difficult to assess the effectiveness of pterins as biomarkers of TBI, specifically neopterin, in their clinical capacity to monitor the severity and progression of injury. (2) The purpose of this review was to evaluate the response of all pterins to mechanical or impact-induced trauma, yet the current literature is severely limited to neopterin studies. Because other pterins like isoxanthopterin, sepiapterin, pterin and xanthopterin have been measured in diseases like cancer [76] and Duchenne muscular dystrophy [68], and these diseases are associated with inflammation, oxidative stress and ischemia, these pterins may also provide some benefit in situations of trauma. Furthermore, the development of novel nanotechnology/biomedical engineering platforms for biomarker discovery in conditions associated with inflammation and oxidative stress [77,78,79] could further enhance the validity and utility of specialist diagnostic biomarkers such as pterins. (3) It was evident that the media used to measure a selected pterin both within and between each of the four categories was different. For example, all exercise-based studies used urine, whereas all surgical studies used plasma or serum. To understand the capacity of pterins to act as diagnostic and prognostic markers, all media should be considered for measurement of pterins.
5. Conclusions
This systematic review evaluated 40 articles that measured pterins in response to mechanical or impact-induced trauma. While neopterin and/or total neopterin were the most quantified pterin, the majority of studies in each of the four categories showed a transient and/or chronic increase. The evidence suggests neopterin and/or total neopterin provide a quality assessment of oxidative stress and inflammation in response to mechanical or impact-induced trauma. Further research on the response of other pterins to mechanical or impact-induced trauma is required before drawing conclusions.
Author Contributions
Conceptualization, A.L., G.B.-P. and S.P.G.; methodology, A.L., G.B.-P. and S.P.G.; formal analysis, A.L., G.B.-P. and S.P.G.; writing—original draft preparation, A.L.; writing—review and editing, A.L., G.B.-P. and S.P.G.; visualization, A.L.
Funding
A.L. was supported by an Alfred Deakin Postdoctoral Research Fellowship. S.P.G’s research has been funded by the Heart Foundation of New Zealand. This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wachter, H.; Fuchs, D.; Hausen, A.; Reibnegger, G.; Werner, E.R. Neopterin as marker for activation of cellular immunity: Immunologic basis and clinical application. Adv. Clin. Chem. 1989, 27, 1–141. [Google Scholar]
- Gieseg, S.P.; Baxter-Parker, G.; Lindsay, A. Neopterin, Inflammation, and Oxidative Stress: What Could We Be Missing? Antioxidants 2018, 7, 80. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, P.F. Tetrahydropterin-Dependent Amino Acid Hydroxylases. Annu. Rev. Biochem. 1999, 68, 355–381. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, F.G. Note on a yellow pigment in butterflies. Nature 1889, 40, 335. [Google Scholar]
- Fuchs, D.; Weiss, G.; Wachter, H. Neopterin, biochemistry and clinical use as a marker for cellular immune reactions. Int. Arch. Allergy Immunol. 1993, 101, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Janmale, T.; Draper, N.; Gieseg, S.P. Measurement of changes in urinary neopterin and total neopterin in body builders using SCX HPLC. Pteridines 2014, 25, 53–63. [Google Scholar] [CrossRef]
- Murr, C.; Fuith, L.C.; Widner, B.; Wirleitner, B.; Baier-Bitterlich, G.; Fuchs, D. Increased neopterin concentrations in patients with cancer: Indicator of oxidative stress? Anticancer Res. 1999, 19, 1721–1728. [Google Scholar] [PubMed]
- Lindsay, A.; Schmiechen, A.; Chamberlain, C.M.; Ervasti, J.M.; Lowe, D.A. Neopterin/7,8-dihydroneopterin is elevated in Duchenne muscular dystrophy patients and protects mdx skeletal muscle function. Exp. Physiol. 2018, 103, 995–1009. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, D.; Chiodi, F.; Albert, J.; Asjö, B.; Hagberg, L.; Hausen, A.; Norkrans, G.; Reibnegger, G.; Werner, E.R.; Wachter, H. Neopterin concentrations in cerebrospinal fluid and serum of individuals infected with HIV-1. AIDS 1989, 3, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Baydar, T.; Yuksel, O.; Sahin, T.T.; Dikmen, K.; Girgin, G.; Sipahi, H.; Kurukahvecioglu, O.; Bostanci, H.; Sare, M. Neopterin as a prognostic biomarker in intensive care unit patients. J. Crit. Care 2009, 24, 318–321. [Google Scholar] [CrossRef]
- Marks, E.C.A.; Wilkinson, T.M.; Frampton, C.M.; Skelton, L.; Pilbrow, A.P.; Yandle, T.G.; Pemberton, C.J.; Doughty, R.N.; Whalley, G.A.; Ellis, C.J.; et al. Plasma levels of soluble VEGF receptor isoforms, circulating pterins and VEGF system SNPs as prognostic biomarkers in patients with acute coronary syndromes. BMC Cardiovasc. Disord. 2018, 18, 169. [Google Scholar] [CrossRef] [PubMed]
- Werner-Felmayer, G.; Golderer, G.; Werner, E.R. Tetrahydrobiopterin Biosynthesis, Utilization and Pharmacological Effects. Curr. Drug Metab. 2002, 3, 159–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenz, A.; Franklin, G.A.; Cheadle, W.G. Systemic inflammation after trauma. Injury 2007, 38, 1336–1345. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.; Henry, A.; Poron, F.; Baba-Amer, Y.; Rooijen, N.; van Plonquet, A.; Gherardi, R.K.; Chazaud, B. Inflammatory monocytes recruited after skeletal muscle injury switch into antiinflammatory macrophages to support myogenesis. J. Exp. Med. 2007, 204, 1057–1069. [Google Scholar] [CrossRef] [Green Version]
- Giannoudis, P. V Current concepts of the inflammatory response after major trauma: An update. Injury 2003, 34, 397–404. [Google Scholar] [CrossRef]
- Sirmali, M.; Türüt, H.; Topçu, S.; Gülhan, E.; Yazici, U.; Kaya, S.; Taştepe, I. A comprehensive analysis of traumatic rib fractures: Morbidity, mortality and management. Eur. J. Cardiothorac. Surg. 2003, 24, 133–138. [Google Scholar] [CrossRef]
- Bauersachs, J.; Schäfer, A. Endothelial dysfunction in heart failure: Mechanisms and therapeutic approaches. Curr. Vasc. Pharmacol. 2004, 2, 115–124. [Google Scholar] [CrossRef]
- Gruen, R.L.; Jurkovich, G.J.; McIntyre, L.K.; Foy, H.M.; Maier, R.V. Patterns of errors contributing to trauma mortality: Lessons learned from 2594 deaths. Ann. Surg. 2006, 244, 371–380. [Google Scholar] [CrossRef]
- Grob, P.; Holch, M.; Fierz, W.; Glinz, W.; Geroulanos, S. Immunodeficiency after major trauma and selective surgery. Pediatr. Infect. Dis. J. 1988, 7, S37–S42. [Google Scholar] [CrossRef]
- Lindsay, A.J.C. Acute and Chronic Individualised Psychophysiological Stress Assessment of Elite Athletes through Non-Invasive Biochemical Analysis. Ph.D. Thesis, University of Canterbury, Christchurch, New Zealand, 2015. [Google Scholar]
- Gunga, H.C.; Machotta, A.; Schobersberger, W.; Mittermayr, M.; Kirsch, K.; Koralewski, E.; Röcker, L. Neopterin, IgG, IgA, IgM, and plasma volume changes during long-distance running. Pteridines 2002, 13, 15–20. [Google Scholar] [CrossRef]
- Lindsay, A.; Lewis, J.; Scarrott, C.; Draper, N.; Gieseg, S.P. Changes in acute biochemical markers of inflammatory and structural stress in rugby union. J. Sports Sci. 2014, 33, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Draper, N.; Lewis, J.G.; Gieseg, S.P.; Gill, N. Positional demands of professional rugby. Eur. J. Sport Sci. 2015, 15, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Lewis, J.; Gill, N.; Gieseg, S.P.; Draper, N. Effect of varied recovery interventions on markers of psychophysiological stress in professional rugby union. Eur. J. Sport Sci. 2015, 15, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Lewis, J.G.; Gill, N.; Gieseg, S.P.; Draper, N. Immunity, inflammatory and psychophysiological stress response during a competition of professional rugby union. Pteridines 2015, 26, 153–160. [Google Scholar] [CrossRef]
- Lindsay, A.; Lewis, J.G.; Scarrott, C.; Gill, N.; Gieseg, S.P.; Draper, N. Assessing the Effectiveness of Selected Biomarkers in the Acute and Cumulative Physiological Stress Response in Professional Rugby Union through Non-invasive Assessment. Int. J. Sports Med. 2015, 36, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Carr, S.; Othman, M.I.; Marks, E.; Davies, S.; Petersen, C.; Draper, N.; Gieseg, S.P. The physiological and mononuclear cell activation response to cryotherapy following a mixed martial arts contest: A pilot study. Pteridines 2015, 26, 143–151. [Google Scholar] [CrossRef]
- Lindsay, A.; Healy, J.; Mills, W.; Lewis, J.G.; Gill, N.; Draper, N.; Gieseg, S.P. Impact-induced muscle damage and urinary pterins in professional rugby: 7,8-dihydroneopterin oxidation by myoglobin. Scand. J. Med. Sci. Sport. 2015, 26, 329–337. [Google Scholar] [CrossRef]
- Lindsay, A.; Othman, M.I.; Prebble, H.; Davies, S.; Gieseg, S.P. Repetitive cryotherapy attenuates the in vitro and in vivo mononuclear cell activation response. Exp. Physiol. Exp. Physiol 2016, 101, 851–865. [Google Scholar] [CrossRef]
- Lindsay, A.; Carr, S.; Cross, S.; Petersen, C.; Lewis, J.G.; Gieseg, S.P. The physiological response to cold-water immersion following a mixed martial arts training session. Appl. Physiol. Nutr. Metab. 2017, 42, 529–536. [Google Scholar] [CrossRef]
- Pilz, G.; Kääb, S.; Kreuzer, E.; Werdan, K. Evaluation of definitions and parameters for sepsis assessment in patients after cardiac surgery. Infection 1994, 22, 8–17. [Google Scholar] [CrossRef]
- Bogă, M.; Islamoğlu, F.; Badak, I.; Cikirikçioğlu, M.; Bakalim, T.; Yağdi, T.; Büket, S.; Hamulu, A. The effects of modified hemofiltration on inflammatory mediators and cardiac performance in coronary artery bypass grafting. Perfusion 2000, 15, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Jerin, A.; Pozar-Lukanovic, N.; Sojar, V.; Stanisavljevic, D.; Paver-Erzen, V.; Osredkar, J. Neopterin—An early marker of surgical stress and hypoxic reperfusion damage during liver surgery. Clin. Chem. Lab. Med. 2002, 40, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.; Eissele, S.; Brückner, U.B.; Gebhard, F.; Becker, H.P. Systemic inflammatory response after endoscopic (TEP) vs Shouldice groin hernia repair. Hernia 2004, 8, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Brkić, K.; Unić, D.; Sutlić, Z.; Biocina, B.; Rudez, I.; Barić, D.; Lukić, I.K. Neopterin kinetics after cardiac surgery with or without cardiopulmonary bypass. Coll. Antropol. 2006, 30, 395–400. [Google Scholar] [PubMed]
- Skrak, P.; Kovacikova, L.; Kunovsky, P. Procalcitonin, neopterin and C-reactive protein after pediatric cardiac surgery with cardiopulmonary bypass. Bratisl. Lek. Listy 2007, 108, 501–505. [Google Scholar] [PubMed]
- Forrest, C.M.; Mackay, G.M.; Oxford, L.; Millar, K.; Darlington, L.G.; Higgins, M.J.; Stone, T.W. Kynurenine metabolism predicts cognitive function in patients following cardiac bypass and thoracic surgery. J. Neurochem. 2011, 119, 136–152. [Google Scholar] [CrossRef] [PubMed]
- Osse, R.J.; Fekkes, D.; Tulen, J.H.M.; Wierdsma, A.I.; Bogers, A.J.J.C.; Mast, R.C.; Hengeveld, M.W. High Preoperative Plasma Neopterin Predicts Delirium After Cardiac Surgery in Older Adults. J. Am. Geriatr. Soc. 2012, 60, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Hol, J.W.; Stolker, R.J.; Klimek, M.; Stronks, D.L.; Fekkes, D. The tryptophan kynurenine pathway, neopterin and IL-6 during vulvectomy and abdominal hysterectomy. J. Biomed. Sci. 2014, 21, 102. [Google Scholar] [CrossRef]
- Berg, K.S.; Stenseth, R.; Pleym, H.; Wahba, A.; Videm, V. Neopterin predicts cardiac dysfunction following cardiac surgery. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Enger, T.B.; Pleym, H.; Stenseth, R.; Greiff, G.; Wahba, A.; Videm, V. A Preoperative Multimarker Approach to Evaluate Acute Kidney Injury After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2017, 31, 837–846. [Google Scholar] [CrossRef] [Green Version]
- Christensen, M.H.E.; Fadnes, D.J.; Røst, T.H.; Pedersen, E.R.; Andersen, J.R.; Våge, V.; Ulvik, A.; Midttun, Ø.; Ueland, P.M.; Nygård, O.K.; et al. Inflammatory markers, the tryptophan-kynurenine pathway, and vitamin B status after bariatric surgery. PLoS ONE 2018, 13, e0192169. [Google Scholar] [CrossRef] [PubMed]
- Baxter-Parker, G.; Roffe, L.; Cross, S.; Frampton, C.; Hooper, G.J.; Gieseg, S.P. Knee replacement surgery significantly elevates the urinary inflammatory biomarkers neopterin and 7,8-dihydroneopterin. Clin. Biochem. 2019, 63, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Lenzlinger, P.M.; Hans, V.H.; Jöller-Jemelka, H.I.; Trentz, O.; Morganti-Kossmann, M.C.; Kossmann, T. Markers for cell-mediated immune response are elevated in cerebrospinal fluid and serum after severe traumatic brain injury in humans. J. Neurotrauma 2001, 18, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Lenzlinger, P.M.; Marx, A.; Trentz, O.; Kossmann, T.; Morganti-Kossmann, M.C. Prolonged intrathecal release of soluble Fas following severe traumatic brain injury in humans. J. Neuroimmunol. 2002, 122, 167–174. [Google Scholar] [CrossRef]
- Brandl, M.; Pscheidl, E.; Amann, W.; Barjasic, A.; Pasch, T. Biochemical and hormonal parameters in patients with multiple trauma. Prog. Clin. Biol. Res. 1989, 308, 743–749. [Google Scholar] [PubMed]
- Krüger, C.; Schütt, C.; Obertacke, U.; Joka, T.; Müller, F.E.; Knöller, J.; Köller, M.; König, W.; Schönfeld, W. Serum CD14 levels in polytraumatized and severely burned patients. Clin. Exp. Immunol. 1991, 85, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Strohmaier, W.; Mauritz, W.; Gaudernak, T.; Grünwald, C.; Schüller, W.; Schlag, G. Septic focus localized by determination of arterio-venous difference in neopterin blood levels. Circ. Shock 1992, 38, 219–221. [Google Scholar] [PubMed]
- Waydhas, C.; Nast-Kolb, D.; Jochum, M.; Trupka, A.; Lenk, S.; Fritz, H.; Duswald, K.H.; Schweiberer, L. Inflammatory mediators, infection, sepsis, and multiple organ failure after severe trauma. Arch. Surg. 1992, 127, 460–467. [Google Scholar] [CrossRef]
- Roumen, R.M.; Redl, H.; Schlag, G.; Zilow, G.; Sandtner, W.; Koller, W.; Hendriks, T.; Goris, R.J. Inflammatory mediators in relation to the development of multiple organ failure in patients after severe blunt trauma. Crit. Care Med. 1995, 23, 474–480. [Google Scholar] [CrossRef]
- Hobisch-Hagen, P.; Wiedermann, F.; Mayr, A.; Fries, D.; Jelkmann, W.; Fuchs, D.; Hasibeder, W.; Mutz, N.; Klingler, A.; Schobersberger, W. Blunted erythropoietic response to anemia in multiply traumatized patients. Crit. Care Med. 2001, 29, 743–747. [Google Scholar] [CrossRef]
- Hensler, T.; Sauerland, S.; Lefering, R.; Nagelschmidt, M.; Bouillon, B.; Andermahr, J.; Neugebauer, E.A.M. The clinical value of procalcitonin and neopterin in predicting sepsis and organ failure after major trauma. Shock 2003, 20, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Egger, G.; Aigner, R.; Glasner, A.; Hofer, H.P.; Mitterhammer, H.; Zelzer, S. Blood polymorphonuclear leukocyte migration as a predictive marker for infections in severe trauma: Comparison with various inflammation parameters. Intensive Care Med. 2004, 30, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.S.; Thavichaigarn, P.; Pattanapanyasat, K.; Siritongtaworn, P.; Kongcharoen, P.; Tongtawe, P.; Yongvanitchit, K.; Jiarakul, N.; Dheeradhada, C.; Pearce, F.J.; et al. Characterization of circulating monocytes expressing HLA-DR or CD71 and related soluble factors for 2 weeks after severe, non-thermal injury. J. Surg. Res. 2005, 129, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Ploder, M.; Pelinka, L.; Schmuckenschlager, C.; Wessner, B.; Ankersmit, H.J.; Fuerst, W.; Redl, H.; Roth, E.; Spittler, A. Lipopolysaccharide-induced tumor necrosis factor alpha production and not monocyte human leukocyte antigen-DR expression is correlated with survival in septic trauma patients. Shock 2006, 25, 129–134. [Google Scholar] [PubMed]
- Ploder, M.; Neurauter, G.; Spittler, A.; Schroecksnadel, K.; Roth, E.; Fuchs, D. Serum phenylalanine in patients post trauma and with sepsis correlate to neopterin concentrations. Amino Acids 2008, 35, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Ploder, M.; Spittler, A.; Schroecksnadel, K.; Neurauter, G.; Pelinka, L.E.; Roth, E.; Fuchs, D. Tryptophan degradation in multiple trauma patients: Survivors compared with non-survivors. Clin. Sci. 2009, 116, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Ploder, M.; Spittler, A.; Kurz, K.; Neurauter, G.; Pelinka, L.E.; Roth, E.; Fuchs, D. Accelerated tryptophan degradation predicts poor survival in trauma and sepsis patients. Int. J. Tryptophan Res. 2010, 3, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.J.; Watne, L.O.; Idland, A.-V.; Raeder, J.; Frihagen, F.; MacLullich, A.M.J.; Staff, A.C.; Wyller, T.B.; Fekkes, D. Cerebrospinal fluid levels of neopterin are elevated in delirium after hip fracture. J. Neuroinflamm. 2016, 13, 170. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.; Bayard, C.; Lepetitcorps, H.; Cohen-Bittan, J.; Appay, V.; Boddaert, J.; Sauce, D. Elevated Neopterin Levels Predict Early Death in Older Hip-fracture Patients. EBioMedicine 2017, 26, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, T.; Nixon, J.C. Analysis of reduced forms of biopterin in biological tissues and fluids. Anal. Biochem. 1980, 102, 176–188. [Google Scholar] [CrossRef]
- Flavall, E.A.; Crone, E.M.; Moore, G.A.; Gieseg, S.P. Dissociation of neopterin and 7, 8-dihydroneopterin from plasma components before HPLC analysis. J. Chromatogr. B 2008, 863, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, D.; Milstien, S.; Krämer, A.; Reibnegger, G.; Werner, E.R.; Goedert, J.J.; Kaufman, S.; Wachter, H. Urinary neopterin concentrations vs total neopterins for clinical utility. Clin. Chem. 1989, 35, 2305–2307. [Google Scholar] [PubMed]
- Allen, D.G.; Whitehead, N.P.; Froehner, S.C. Absence of Dystrophin Disrupts Skeletal Muscle Signaling: Roles of Ca2+, Reactive Oxygen Species, and Nitric Oxide in the Development of Muscular Dystrophy. Physiol. Rev. 2016, 96, 253–305. [Google Scholar] [CrossRef] [PubMed]
- Bayır, H.; Kochanek, P.M.; Kagan, V.E. Oxidative Stress in Immature Brain after Traumatic Brain Injury. Dev. Neurosci. 2006, 28, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Gelman, S.I. Disturbances in Hepatic Blood Flow During Anesthesia and Surgery. Arch. Surg. 1976, 111, 881. [Google Scholar] [CrossRef] [PubMed]
- Van der Bilt, J.D.W.; Borel Rinkes, I.H.M. Surgery and angiogenesis. Biochim. Biophys. Acta Rev. Cancer 2004, 1654, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; McCourt, P.M.; Karachunski, P.; Lowe, D.A.; Ervasti, J.M. Xanthine oxidase is hyper-active in Duchenne muscular dystrophy. Free Radic. Biol. Med. 2018, 129, 364–371. [Google Scholar] [CrossRef] [PubMed]
- McLellan, C.P.; Lovell, D.I.; Gass, G.C. Biochemical and endocrine responses to impact and collision during elite rugby league match play. J. Strength Cond. Res. 2011, 25, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Carr, S.; Draper, N.; Gieseg, S.P. Urinary myoglobin quantification by high-performance liquid chromatography: An alternative measurement for exercise-induced muscle damage. Anal. Biochem. 2015, 491, 37–42. [Google Scholar] [CrossRef]
- Cunniffe, B.; Hore, A.J.; Whitcombe, D.M.; Jones, K.P.; Baker, J.S.; Davies, B. Time course of changes in immuneoendocrine markers following an international rugby game. Eur. J. Appl. Physiol. 2010, 108, 113–122. [Google Scholar] [CrossRef]
- Asimakopoulos, G. Systemic inflammation and cardiac surgery: An update. Perfusion 2001, 16, 353–360. [Google Scholar] [CrossRef]
- Morganti-Kossmann, M.C.; Rancan, M.; Stahel, P.F.; Kossmann, T. Inflammatory response in acute traumatic brain injury: A double-edged sword. Curr. Opin. Crit. Care 2002, 8, 101–105. [Google Scholar] [CrossRef]
- Cornelius, C.; Crupi, R.; Calabrese, V.; Graziano, A.; Milone, P.; Pennisi, G.; Radak, Z.; Calabrese, E.J.; Cuzzocrea, S. Traumatic Brain Injury: Oxidative Stress and Neuroprotection. Antioxid. Redox Signal. 2013, 19, 836–853. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Lingsma, H.F. ALERT-TBI study on biomarkers for TBI: Has science suffered? Lancet Neurol. 2018, 17, 737–738. [Google Scholar] [CrossRef]
- Burton, C.; Shi, H.; Ma, Y. Normalization of urinary pteridines by urine specific gravity for early cancer detection. Clin. Chim. Acta 2014, 435, 42–47. [Google Scholar] [CrossRef]
- Ganau, L.; Prisco, L.; Ligarotti, G.K.I.; Ambu, R.; Ganau, M. Understanding the Pathological Basis of Neurological Diseases Through Diagnostic Platforms Based on Innovations in Biomedical Engineering: New Concepts and Theranostics Perspectives. Medicines 2018, 5, 22. [Google Scholar] [CrossRef]
- Ganau, M.; Paris, M.; Syrmos, N.; Ganau, L.; Ligarotti, G.K.I.; Moghaddamjou, A.; Prisco, L.; Ambu, R.; Chibbaro, S. How Nanotechnology and Biomedical Engineering Are Supporting the Identification of Predictive Biomarkers in Neuro-Oncology. Medicines 2018, 5, 23. [Google Scholar] [CrossRef]
- Ganau, M.; Syrmos, N.; Paris, M.; Ganau, L.; Ligarotti, G.K.I.; Moghaddamjou, A.; Chibbaro, S.; Soddu, A.; Ambu, R.; Prisco, L. Current and Future Applications of Biomedical Engineering for Proteomic Profiling: Predictive Biomarkers in Neuro-Traumatology. Medicines 2018, 5, 19. [Google Scholar] [CrossRef]
Figure 1.
A flow diagram detailing the inclusion/exclusion identification of studies in this systematic review.
Figure 1.
A flow diagram detailing the inclusion/exclusion identification of studies in this systematic review.

Figure 2.
(A) Percent of studies that measured an increase, decrease or no change, or did not state or measure changes in pterins. (B) Studies that reported a change in pterin concentration within 24 hours of trauma or (C) greater than 48 hours post-trauma.
Figure 2.
(A) Percent of studies that measured an increase, decrease or no change, or did not state or measure changes in pterins. (B) Studies that reported a change in pterin concentration within 24 hours of trauma or (C) greater than 48 hours post-trauma.


{kind=link}
{kind=link}
Table 1.
Studies measuring pterins following impact-induced trauma in exercise and sport.
| Authors | Year | Pterin | Media | Population | Intervention | Outcome |
|---|---|---|---|---|---|---|
| Lindsay et al. [22] | 2015 | NP and Total NP | Urine corrected with specific gravity | Elite amateur rugby players; n = 11; median height = 1.87 m; median weight = 96 kg | Rugby game | - NP ↑ (p = 0.02) - Total NP ↑ (p = 0.008) - Both ↑ within 60 min post-game and retuned to baseline within 17 h and remained until 86 h |
| Lindsay et al. [23] | 2015 | Total NP | Urine corrected with specific gravity | Professional rugby players; n = 37; height = 1.81– 2.01 m; weight = 92.9– 112.3 kg; age = 23.7–27.5 years | Several rugby games separated by player position | ↑ (43.6–109.6%) within 60 min post-game |
| Lindsay et al. [24] | 2015 | Total NP | Urine corrected with specific gravity | Professional rugby players; n = 37; height = 1.86 ± 0.07 m; weight = 104.5 ± 9.3 kg; age = 26 ± 3.5 years | Rugby game – data from several games compiled together during a season | ↑ (64%) within 60 min post-game. Still significantly elevated 36 hours post-game |
| Lindsay et al. [25] | 2015 | Total NP | Urine corrected with specific gravity | Professional rugby players; n = 37; height = 1.86 ± 0.07 m; weight = 104.5 ± 9.3 kg; age = 26 ± 3.5 years | Rugby season (20 weeks) | No change throughout the season |
| Lindsay et al. [26] | 2015 | NP and Total NP | Urine corrected with specific gravity | Semi-professional rugby players; n = 24; height = 1.87 ± 0.06 m; weight = 103.3 ± 11.6 kg; age = 24.2 ± 2.9 years | Three rugby games separated by a week | - NP ↑ (p < 0.002) - Total NP ↑ (1.96–2.41 fold; p ≤ 0.003) - Both positively correlated with number of impacts Both ↑ immediately post-each game |
| Lindsay et al. [27] | 2015 | NP and Total NP | Urine corrected with specific gravity | Semi-professional MMA; n = 10; height = 1.77 ± 0.04 m; weight = 79.5 ± 0.5 kg; age = 27.3 ± 3.3 years | MMA fight | - NP ↑ (p = 0.02) 1 h post-fight but was not different up to 48 hours post - Total NP did not change |
| Lindsay et al. [28] | 2016 | NP, 7,8-NP, BP, Total BP, XP | Urine corrected with specific gravity | Professional rugby players; n = 14–23; height = 1.86 ± 0.07 m; weight = 104.5 ± 9.3 kg; age = 26 ± 3.5 years | Rugby game—four separate games separated by a week | - NP ↑ (1.37–2.82 fold) - Total NP ↑ (1.45–1.89 fold) - BP ↑ (1.28–1.36 fold) - Total BP ↑ (1.49–1.85 fold) - XP ↑ (0.84–1.57 fold) - All ↑ within 90 min post-game |
| Lindsay et al. [29] | 2016 | NP and Total NP | Urine corrected with specific gravity | Semi-professional MMA; n = 14; height = 1.78 ± 0.08 m; weight = 84.3 ± 12.9 kg; age = 26.6 ± 8.2 years | Six-week MMA training camp | NP and Total NP ↑ (p < 0.05–0.001) throughout the 6-week training duration |
| Lindsay et al. [30] | 2017 | NP and Total NP | Urine corrected with specific gravity | Semi-professional MMA; n = 15; height = 1.8 ± 0.09 m; weight = 88.8 ± 14.5 kg; age = 28.3 ± 5.7 years | MMA training session | - NP ↑ 4.07 fold and remained elevated up to 24 hours post - Total NP ↑ 3.15 fold and remained elevated 24 hours post |
BP; biopterin, MMA; mixed martial arts or artists, NP; Neopterin, Total BP; BP + BH2 (7,8-dihydrobiopterin) + BH4 (5,6,7,8-tetrahydrobiopterin), Total NP; NP + 7,8-dihydroneopterin, XP; xanthopterin.
Table 2.
Studies measuring pterins following surgery.
| Authors | Year | Pterin | Media | Population | Categorization | Outcome |
|---|---|---|---|---|---|---|
| Grob et al. [19] | 1988 | NP | Serum | Consecutive patients hospitalised for selective surgery; n = 35/surgery (10 females and 25 males); age 18–72 years | Herniotomy, cholecystectomy, major surgery on rectum or colon, aorto-coronary bypass or ypsilon graft | No change within 4-days post-surgery among all surgery types |
| Pilz et al. [31] | 1994 | NP | Plasma | Patients excluding heart transplantation and pacemaker implantation; n = 110; age = 58.4 ± 1.1 (no complications) and 61.0 ± 2.3 (septic complication) | Elective cardiac surgery | - ↑ after day 1 and remained elevated after 3 days - Delayed ↑ after extracorporeal circulation - Greater ↑ in septic complication patients post-surgery |
| Bogă et al. [32] | 2000 | NP | Plasma | Patients excluding those undergoing emergency surgery, or having a diagnosed systemic disorder such as hemostatic defect, hypertension, diabetes or renal failure; n = 40 (10 female and 30 male); age = 57.8 ± 8.9 (study group) and 61.2 ± 7.5 years (control group) | Coronary artery bypass grafting—with or without ultrafiltration | - mean NP ↓ after surgery and ↑ 3- and 20-hours post-surgery (statistical analysis not provided) - no difference with ultrafiltration |
| Jerin et al. [33] | 2002 | NP | Serum | Patients suffered from malignant disease (hepatic metastases of colonic cancer, hepatocellular cancer, gallbladder cancer or cholangiocarcinoma) or non-malignant disease (echinococcus cysts, liver haemangioma, liver adenoma or Carroli disease); n = 27 (16 female and 11 male); age 5–77 years | Liver resection | - No change 24-hours post-surgery - NP higher in patients with malignant disease. |
| Schwab et al. [34] | 2004 | NP | Serum | No exclusions; n = 101; height = 162– 196 cm; weight = 53–108 kg; age = 18–90 years | Hernia surgery—local or general anaesthetic and either unilateral or bilateral repair | NP ↑ significantly 1 h post-surgery but no difference between the surgical groups. NP was still elevated 72 hours post-surgery |
| Brkić et al. [35] | 2006 | NP | Serum | Patients excluding those undergoing reoperations, combined procedures or emergency surgery, those with acute or chronic renal failure requiring hemodialysis and known inflammatory diseases requiring antibiotics or steroids; n = 78 (21 female and 57 male); age = 56–68 years | Cardiac surgery with or without cardiopulmonary bypass | - Both surgeries ↑ NP at 24 and 72 h post-surgery with bypass further ↑ concentrations - NP correlated with ICU stay duration |
| Skrak et al. [36] | 2007 | NP | Serum | Patients with a congenital heart defect; n = 152; age = 11 days–13 years; weight = 3.3–44 kg | Cardiac surgery with cardiopulmonary bypass | NP ↑ in neonates and infants/children after one day and remained elevated after 2 days |
| Forrest et al. [37] | 2011 | NP | Serum | No data on inclusion – control group were major non-thoracic surgery patients; n = 28 (3 female and 25 male); age = 60.2 ± 1.7 years | Cardiac bypass surgery | - Cardiac surgery ↓ NP compared to baseline but ↑ 6 days-post - Thoracic surgery did not affect NP |
| Osse et al. [38] | 2012 | Total NP BH4 | Plasma | Patients excluding those whom required deep cooling, circulatory arrest, or emergency surgery; n = 125 provided pterin samples; median age = 76 years | Cardiac surgery—coronary artery bypass graft or valve surgery | - NP ↑ following surgery. Elevated pre-surgical NP associated with a greater risk of becoming delirious after surgery - BH4 did not change or correlate with development of delirium |
| Hol et al. [39] | 2014 | Total NP | Plasma | Patients > 18 years of age and ASA classification I-III; n = 28 (all female);age = 62 ± 12 and 44 ± 9 years; height = 166 ± 5 and 167 ± 6 cm; weight = 71 ± 10 and 71 ± 7 | Vulvectomy or abdominal hysterectomy | - Surgery ↓ total NP for both surgical groups up to 24 hours post - Vulvectomy patients had higher concentrations pre and post-surgery |
| Berg et al. [40] | 2015 | NP | Plasma | Patients excluding those with infectious blood, active endocarditis, underwent off-pump surgery, intercurrent infection or elevated levels of CRP; n = 1018 (282 female and 736 male); age = 67–75 years | Cardiac surgery | Improved the accuracy of predicting cardiac dysfunction after surgery |
| Enger et al. [41] | 2017 | NP | Plasma | Patients without preoperative dialysis or missing serum creatinine; n = 1015 (282 female and 733 male);age = 66–76 years;body mass index = 26.6–29.4 kg/m2 | Cardiac surgery with cardiopulmonary bypass | Independent predictor of CSA-AKI |
| Christensen et al. [42] | 2018 | NP | Plasma | Patients had at least one obesity related comorbidity (such as T2D, hypertension or dyslipidaemia); n = 37 (25 females and 12 males);age = 42.5–53.5 years;body mass index = 40.9–47.6 | Laparoscopic sleeve gastrectomyor biliopancreatic diversion with duodenal switch | No change up to 12 months post-surgery |
| Baxter-Parker et al. [43] | 2019 | NP and Total NP | Urine | Patients were excluded if below 18 or above 80 years of age, smokers, or patients having recently received a diagnosis of cancer.; n = 19; age = 62.68 ± 8.97 years. Control subjects; n = 20; age = 37.7 ± 12.9 | Knee replacement surgery | - NP ↑ two days post-surgery - Total NP did not change in surgical group - NP and total NP elevated versus control 2- and 1-days following surgery, respectively |
ASA; American Society of Anesthesiologists, BH4 (5,6,7,8-tetrahydrobiopterin), CRP; C-reactive protein, CSA-AKI; acute kidney injury following cardiac surgery, NP; Neopterin, T2D; type 2 diabetes, Total BP; BP + BH2 (7,8-dihydrobiopterin) + BH4 (5,6,7,8-tetrahydrobiopterin), Total NP; NP + 7,8-dihydroneopterin.
Table 3.
Studies measuring pterins following traumatic brain injury.
| Authors | Year | Pterin | Media | Population | Categorization | Outcome |
|---|---|---|---|---|---|---|
| Lenzlinger et al. [44] | 2001 | NP | CSF and Serum | Patients presented with a Glasgow Coma Score at admission equal to or less than 8 and/or abnormalities in the computer aided tomography of the brain; n = 41 (9 female and 32 male); age 38 ± 17 years | Isolated TBI | - CSF NP ↑ in 78% of patients and remained elevated 21 days post-surgery (1.88–39.48 ng/mL) - Serum NP ↑ in 73% of patients and remained elevated 14 days post-surgery (0.59–40.05 ng/mL) |
| Lenzlinger et al. [45] | 2002 | NP | CSF | Patients had a Glasgow Coma Scale (GCS) score equal to or less than 8 at admission and alterations in the computer aided tomography; n = 10 (4 female and 6 male); age 18–65 years | Severe TBI | No directly stated values but examination of the results suggest values ranged from approximately 0–40 ng/mL |
CSF; cerebrospinal fluid, NP; Neopterin, TBI; traumatic brain injury.
Table 4.
Studies measuring pterins following multiple trauma or bone fracture.
| Authors | Year | Pterin | Media | Population | Categorization | Outcome |
|---|---|---|---|---|---|---|
| Brandl et al. [46] | 1989 | NP | Serum | Injures were initially quantified according to the ISS; n = 51 but NP measured in 26 | Multiple-trauma | NP higher in non-survivors |
| Krüger et al. [47] | 1991 | NP | Serum | Patients had no acute disease process prior to trauma. All patients had multiple fractures of the extremities, blunt trauma, and a hypovolaemic shock. The Glasgow coma score was above 8 points within 6 h post trauma n = 16; age 36 ± 17 years | Polytrauma | NP ↑ after trauma (values not provided) |
| Strohmaier et al. [48] | 1992 | NP | Plasma | Case study—38-year-old female with ISS of 66 | Trauma-accident victim—leg amputation | NP ↑ during the clinical course |
| Waydhas et al. [49] | 1992 | NP | Plasma | Patients admitted to the emergency department with less than 6 hours between accident and admission to the emergency department; between 16 and 70 years of age; and severe injuries of at least two body regions (head/brain, thorax, abdomen, skeletal system) or three major fractures (ISS ≥ 32; n = 100 (36 female and 74 male); age = 38 years | Trauma | - NP ↑ within 24 h - NP higher in non-survivors from 2 days post-admission - NP higher in surviving patients with organ failure |
| Roumen et al. [50] | 1995 | NP | Urine (creatinine standardized) | Patients were included in the study if the ISS was ≥ 33; n = 56 | Multiple trauma | NP higher in patients with multiple organ failure once it had become established 8–10 days post-trauma |
| Hobisch-Hagen et al. [51] | 2001 | NP | Serum | Patients aged >19 yrs, expected, stay in the ICU > 72 h Partial pressure of oxygen (PaO2) > 75 torr during the ICU stay, no renal or hepatic failure, no history of hematopoietic or endocrinological disorder, and ISS ≥ 30; n = 23 (5 female and 18 male); age = 19–59 years | Multiple mechanical trauma | NP low after admission but ↑ until 9 days post-trauma |
| Hensler et al. [52] | 2003 | NP | Plasma | Patients were ≥ 16 years of age, ISS ≥ 16 and an expected minimum of survival for ≥ 3 days. Patients with acquired or inherited immunodeficiencies and patients receiving immunosuppressive therapy were excluded; n = 137 (35 female and 102 male); age = 38.5 ± 16.6 years | Trauma, including brain injury | - NP ↓ post-trauma and ↑ 1- and 2-days post - NP not a predictor of patients developing sepsis or multi-organ failure |
| Egger et al. [53] | 2004 | NP | Blood – not specified | Patients who died or who were transported abroad where the further course could not be followed were excluded from the study. Eight patients with an ISS of ≤ 20, 10 patients with an ISS of 21–30, and eight patients with an ISS > 30 were included; n = 26 (8 female and 18 male); age = 17–77 years; | Multiple trauma | - NP ↑ in some patients (unclear at what time point) - NP correlated with the severity of trauma |
| Walsh et al. [54] | 2005 | NP | Urine (creatinine standardized) | Patients aged 18 to 50 with an ISS > 20 were included. Patients that received corticosteroids for head injuries or died within 1 week from severe mechanical injury were excluded | Severe injury | - mean NP ↑ 1-day post-trauma - NP ↑ in the 13 days post-injury and was higher in patients developing sepsis |
| Ploder et al. [55] | 2006 | NP | Plasma | Patients were aged between 18 and 80 years and multiple trauma, defined as injury to two or more anatomic areas (head, chest, abdomen, or pelvis) or to one anatomic area and to two long bones (femur, tibia, or humerus). Exclusion criteria were isolated head injury, known immunosuppressive therapy, or known HIV infection; n = 21; age = 38.7 ± 15.8 years. Mean ISS = 40.6 ± 11.6 | Multiple trauma | NP continually increased above entry to ICU for 14 days and was higher in non-survivors |
| Ploder et al. [56] | 2008 | NP | Serum | Patients with an APACHE score of 18.9 ± 6.75 and ISS score of 39 ± 13.1; n = 18 (4 female and 14 male); age = 45 ± 19 years. | Trauma | - NP ↑ in patients with 79.8% above the 95th percentile of healthy controls - NP and APACHE scores correlate 4-days post-trauma |
| Ploder et al. [57] | 2009 | NP | Serum | Patients aged between 22 - 77 years and evidence of a multiple trauma (ISS = 39.1 ± 13.1; APACHE = 17.5 ± 6.5). Exclusion criteria were known immunosuppressive therapy, known HIV infection or any other chronic disease; n = 15 (3 female and 12 male); age = 40.4 ± 17.2 years | Trauma | - NP ↑ compared to controls - NP greater in patients who died during follow-up (7–37-days post-trauma) |
| Ploder et al. [58] | 2010 | NP | Plasma | Patients admitted to ICU. APACHE score: 18.9 ± 6.75, ISS: 39 ± 13.1; n = 18 (4 female and 14 male); age = 45 ± 19 years | Trauma | ↑ NP compared to control subjects but timeline could not be determined |
| Hall et al. [59] | 2016 | Total NP | CSF and serum | Patients included if the fracture was caused by a low energy trauma (defined as a fall from less than 1 meter). Patients were excluded if they were under the age of 60, were nursing home residents, had significant Parkinson’s disease or had malignant or other comorbid disease such that prognosis was less than one year; n = 139 | Hip fracture | - NP values above upper end of normal - NP highest in patients with delirium and/or cognitive impairment |
| Larsen et al. [60] | 2017 | NP | Plasma | Patients aged 75 years and older, free of medication and diseases affecting the immune system (e.g., cancers, autoimmune disorders), absence of prior physical disabilities and, absence of cognitive disorders; n = 60 | Hip fracture followed by surgery | Predictor of mortality one-year post-fracture and correlates negatively with time of survival after fracture surgery |
CRP; C-reactive protein, CSF; cerebrospinal fluid, HIV; human-immunodeficiency virus, ICU; intensive care unit, ISS; injury severity score, NP; Neopterin, T2D; type 2 diabetes, Total NP; NP + 7,8-dihydroneopterin.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lindsay, A.; Baxter-Parker, G.; Gieseg, S.P. Pterins as Diagnostic Markers of Mechanical and Impact-Induced Trauma: A Systematic Review. J. Clin. Med. 2019, 8, 1383. https://doi.org/10.3390/jcm8091383
AMA Style
Lindsay A, Baxter-Parker G, Gieseg SP. Pterins as Diagnostic Markers of Mechanical and Impact-Induced Trauma: A Systematic Review. Journal of Clinical Medicine. 2019; 8(9):1383. https://doi.org/10.3390/jcm8091383
Chicago/Turabian StyleLindsay, Angus, Gregory Baxter-Parker, and Steven P. Gieseg. 2019. "Pterins as Diagnostic Markers of Mechanical and Impact-Induced Trauma: A Systematic Review" Journal of Clinical Medicine 8, no. 9: 1383. https://doi.org/10.3390/jcm8091383
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.