How the New European Union’s (Pictorial) Tobacco Health Warnings Influence Quit Attempts and Smoking Cessation: Findings from the 2016–2017 International Tobacco Control (ITC) Netherlands Surveys

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Attrition Analyses
3.2. Sample Characteristics
3.3. Correlations
3.4. Structural Equation Model
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Union. Gecombineerde Gezondheidswaarschuwingen Voor Roken Bestemde Tabaksproducten. 2015. Available online: https://ec.europa.eu/health/sites/health/files/tobacco/docs/healthwarnings_netherlands.pdf (accessed on 11 September 2019).
- European Union (EU). Directive 2014/40/EU of the European Parliament and of the council of 3 April 2014 on the approximation of the laws, regulations and administrative provisions of the member states concerning the manufacture, presentation and sale of tobacco and related products and repealing Directive 2001/37/EC. Off. J. Eur. Union 2014, L127, 1–38. [Google Scholar]
- Hammond, D. Health warning messages on tobacco products: A review. Tob. Control 2011, 20, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Noar, S.M.; Francis, D.B.; Bridges, C.; Sontag, J.M.; Ribisl, K.M.; Brewer, N.T. The impact of strengthening cigarette pack warnings: Systematic review of longitudinal observational studies. Soc. Sci. Med. 2016, 164, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Monárrez-Espino, J.; Liu, B.; Greiner, F.; Bremberg, S.; Galanti, R. Systematic Review of the Effect of Pictorial Warnings on Cigarette Packages in Smoking Behavior. Am. J. Public Health 2014, 104, e11–e30. [Google Scholar] [CrossRef]
- Canadian Cancer Society. Cigarette Package Health Warnings. International Status Report, 6th ed.; Canadian Cancer Society: Toronto, ON, Canada, 2018; Available online: https://www.tobaccofreekids.org/assets/global/pdfs/en/WL_status_report_en.pdf. (accessed on 5 May 2019).
- Department of Health and Human Services (DHHS). The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24455788. (accessed on 1 November 2019).
- GBD 2015 Tobacco Collborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef]
- Goodchild, M.; Nargis, N.; Tursan d’Espaignet, E. Global economic cost of smoking attributable diseases. Tob. Control 2017, 27, 58–64. [Google Scholar] [CrossRef]
- Yong, H.-H.; Borland, R.; Thrasher, J.F.; Thompson, M.E.; Nagelhout, G.E.; Fong, G.T.; Hammond, D.; Cummings, M.K. Mediational pathways of the impact of cigarette warning labels on quit attempts. Health Psychol. 2014, 33, 1410–1420. [Google Scholar] [CrossRef]
- Fong, G.T.; Cummings, K.M.; Borland, R.; Hastings, G.; Hyland, A.; Giovino, G.A.; Hammond, D.; Thomposn, M.E. The conceptual framework of the International Tobacco Control (ITC) Policy Evaluation Project. Tob. Control 2006, 15, iii3–iii11. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- De Vries, H. An integrated approach for understanding health behavior; the I-Change Model as an example. Int. J. Psychol. Behav. Sci. 2017, 2, 555–585. [Google Scholar] [CrossRef]
- Dohnke, B.; Weiss-Gerlach, E.; Spies, C.D. Social influences on the motivation to quit smoking: Main and moderating effects of social norms. Addict. Behav. 2011, 36, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Topa, G.; Moriano, J.A. Theory of planned behavior and smoking: Meta-analysis and SEM model. Subst. Abuse Rehabil. 2010, 1, 23–33. [Google Scholar] [CrossRef] [PubMed]
- De Vries, H.; Dijkstra, M.; Kuhlman, P. Self-efficacy: The third factor besides attitude and subjective norm as a predictor of behavioural intentions. Health Educ. Res. 1988, 3, 273–282. [Google Scholar] [CrossRef]
- Schoenaker, D.A.; Brennan, E.; Wakefield, M.A.; Durkin, S.J. Anti-smoking social norms are associated with increased cessation behaviours among lower and higher socioeconomic status smokers: A population-based cohort study. PLoS ONE. 2018, 13, e0208950. [Google Scholar] [CrossRef]
- O’callaghan, F.V.; Callan, V.J.; Baglioni, A. Cigarette use by adolescents: Attitude behavior relationships. Subst. Use Misuse 1999, 34, 455–468. [Google Scholar] [CrossRef]
- Miller, C.L.; Hill, D.J.; Quester, P.G.; Hiller, J.E. The impact of Australia’s new graphic cigarette packet warnings on smokers’ beliefs and attitudes. Australas. Mark. J. 2011, 19, 181–188. [Google Scholar] [CrossRef]
- Vangeli, E.; Stapleton, J.; Smit, E.S.; Borland, R.; West, R. Predictors of attempts to stop smoking and their success in adult general population samples: A systematic review. Addiction 2011, 106, 2110–2121. [Google Scholar] [CrossRef]
- Borland, R.; Wilson, N.; Fong, G.T.; Hammond, D.; Cummings, K.M.; Yong, H.-H.; Hosking, W.; Hastings, G.; Thrasher, J.; McNeill, A. Impact of graphic and text warnings on cigarette packs: Findings from four countries over five years. Tob. Control 2009, 18, 358–364. [Google Scholar] [CrossRef]
- Green, A.C.; Kaai, S.C.; Fong, G.T.; Driezen, P.; Quah, A.C.K.; Burhoo, P. Investigating the effectiveness of pictorial health warnings in Mauritius: Findings from the ITC Mauritius Survey. Nicotine Tob. Res. 2014, 16, 1240–1247. [Google Scholar] [CrossRef]
- Yong, H.-H.; Fong, G.T.; Driezen, P.; Borland, R.; Quah, A.C.K.; Sirirassamee, B.; Hamann, S.; Omar, M. Adult smokers’ reactions to pictorial health warning labels on cigarette packs in Thailand and moderating effects of type of cigarette smoked: Findings from the International Tobacco Control Southeast Asia Survey. Nicotine Tob. Res. 2013, 15, 1339–1347. [Google Scholar] [CrossRef]
- Nagelhout, G.E.; Willemsen, M.C.; de Vries, H.; Mons, U.; Hitchman, S.C.; Kunst, A.E.; Guignard, R.; Siahpush, M.; Yong, H.H.; van den Putte, B.; et al. Educational differences in the impact of pictorial cigarette warning labels on smokers: Findings from the International Tobacco Control (ITC) Europe surveys. Tob. Control 2015, 25, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Yong, H.-H.; Wilson, N.; Fong, G.T.; Hammond, D.; Cummings, K.M.; Hosking, W.; McNeill, A. How reactions to cigarette packet health warnings influence quitting: Findings from the ITC Four-Country survey. Addiction 2009, 104, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.; Fong, G.T.; McDonald, P.W.; Brown, K.S.; Cameron, R. Graphic Canadian cigarette warning labels and adverse outcomes: Evidence from Canadian smokers. Am. J. Public Health 2004, 94, 1442–1445. [Google Scholar] [CrossRef] [PubMed]
- Nagelhout, G.E.; Willemsen, M.C.; Thompson, M.E.; Fong, G.T.; van den Putte, B.; de Vries, H. Is web interviewing a good alternative to telephone interviewing? Findings from the International Tobacco Control (ITC) Netherlands Survey. BMC Public Health 2010, 10, 351. [Google Scholar] [CrossRef]
- Hyland, A.; Borland, R.; Li, Q.; Yong, H.H.; McNeill, A.; Fong, G.T.; O’Connor, R.J.; Cummings, K.M. Individual-level predictors of cessation behaviours among participants in the International Tobacco Control (ITC) Four Country Survey. Tob. Control 2006, 15, iii83–iii94. [Google Scholar] [CrossRef]
- Diamantopoulos, A.; Winklhofer, H.M. Index construction with formative indicators: An alternative to scale development. J. Mark. Res. 2001, 38, 269–277. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Rickert, W.; Robinson, J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Addiction 1989, 84, 791–800. [Google Scholar] [CrossRef]
- Driezen, P.; Thompson, M. Comparing Policy Measures across Multple ITC Countries: Adjusting for Time-in Sample. 2011. Available online: http://www.itcproject.org/files/ITC_Technical_Report_time-in-sample adjustment_Dec2011.pdf (accessed on 12 January 2018).
- Enders, C. Applied Missing Data Analysis; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Raghunathan, T.E.; Lepkowski, J.M.; van Hoewyk, J.; Solenberger, P. A multivariate technique for multiply imputing missing values using a sequence of regression models. Surv. Methodol. 2001, 27, 85–96. [Google Scholar]
- Van Buuren, S.; Brand, J.P.; Groothuis-Oudshoorn, C.G.; Rubin, D.B. Fully conditional specification in multivariate imputation. J. Stat. Comput. Simul. 2006, 76, 1049–1064. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V.A. Comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Carlin, J.B. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat. Med. 2010, 29, 2920–2931. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; Bechger, T.M. An introduction to structural equation modeling. Fam. Sci. Rev. 1998, 11, 354–373. [Google Scholar]
- Silpasuwan, P.; Ngoenwiwatkul, Y.; Viwatwongkasem, C.; Satitvipawee, P.; Sirichotiratana, N.; Sujirarat, D. Potential effectiveness of health warning labels among employees in Thailand. J. Med. Assoc. Thail. 2008, 91, 551–558. [Google Scholar]
- Noar, S.M.; Hall, M.G.; Francis, D.B.; Ribisl, K.M.; Pepper, K.M.; Brewer, N.T. Pictorial cigarette pack warnings: A meta-analysis of experimental studies. Tob. Control 2015, 25, 341–354. [Google Scholar] [CrossRef]
- Hammond, D.; Fong, G.T.; McNeill, A.; Borland, R.; Cummings, K.M. Effectiveness of cigarette warning labels in informing smokers about the risks of smoking: Findings from the International Tobacco Control (ITC) Four Country Survey. Tob. Control 2006, 15, iii19–iii25. [Google Scholar] [CrossRef]
- Strahan, E.J.; White, K.; Fong, G.T.; Fabrigar, L.R.; Zanna, M.P.; Cameron, R. Enhancing the effectiveness of tobacco package warning labels: A social psychological perspective. Tob. Control 2002, 11, 183–190. [Google Scholar] [CrossRef]
- Moodie, C.; Angus, K.; Stead, M.; Bauld, L. Plain Tobacco Packaging Research: An Update. 2013. Available online: https://dspace.stir.ac.uk/bitstream/1893/24418/1/Moodie_et_al_2013_PlainPacks_update.pdf (accessed on 5 May 2019).
- Gwaltney, C.J.; Metrik, J.; Kahler, C.W.; Shiffman, S. Self-efficacy and smoking cessation: A meta-analysis. Psychol. Addict. Behav. 2009, 23, 56–66. [Google Scholar] [CrossRef]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G.; Gottlieb, N.H.; Fernández, M.E. Planning Health Promotion Programs, 3rd ed.; Jossey-Bass: San Fransisco, CA, USA, 2010. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Outcome | Question Wording and Response Options |
|---|---|
| Policy specific variable (Wave 10) | |
| Health warning salience | 1. In the last 30 days, how often, if at all, have you noticed photos on cigarette packages or on roll-your-own packs?—(1) Never, (2) Rarely, (3) Sometimes, (4) Often, (5) Very Often, or Don’t know (coded as missing) |
| 2. In the last 30 days, how often, if at all, have you read or looked closely at the photos on cigarette packages or on roll-your-own packs?—(1) Never, (2) Rarely, (3) Sometimes, (4) Often, (5) Very Often, or Don’t know (coded as missing) | |
| Psychosocial mediators (Wave 10) | |
| Attitude towards quitting smoking | If you quit smoking within the next six months, this would be. 1. (1) Very foolish, (2) Foolish, (3) Not sensible and not foolish, (4) Wise, sensible, (5) Very wise and sensible or Don’t know (coded as missing) |
| 2. (1) Very disagreeable (2) Disagreeable (3) Not agreeable, but also not disagreeable, (4) Agreeable (5) Very agreeable (pleasant, gratifying), or Don’t know (coded as missing) | |
| 3. (1) Very negative, (2) Negative, (3) Not positive and not negative, (4) Positive, (5) Very positive, or Don’t know (coded as missing) | |
| Perceived social norms towards quitting | Thinking about the people who are important to you—how do you think most of them would feel about your quitting smoking within the next six months?—(1) Strongly disapprove, (2) Disapprove, (3) Neutral, (4) Approve, (5) Strongly approve, or Don’t know (coded as missing) |
| Self-efficacy to quit smoking | 1. If you decided to give up smoking completely in the next six months, how sure are you that you would succeed?—(1) Not at all sure, (2) Slightly sure, (3) Moderately sure, (4) Very sure, (5) Extremely sure, or Don’t know (coded as missing) |
| 2. How easy or hard would it be for you to quit smoking if you wanted to?—(1) Extremely difficult, (2) Very difficult, (3) Moderately difficult, (4) Slightly difficult, (5) Not at all difficult, or Don’t know (coded as missing) | |
| Health worries | How worried are you, if at all, that smoking will damage your health in the future?—(1) Not at all worried, (2) A little worried, (3) Moderately worried, (4) Very worried, or Don’t know (coded as missing) |
| Knowledge | Based on what you know or believe, does smoking cause… 1. Lung cancer—(0) No, (1) Yes, Don’t know (0) 2. Heart disease—(0) No, (1) Yes, Don’t know (0) 3. Impotence in male smokers—(0) No, (1) Yes, Don’t know (0) 4. Blindness—(0) No, (1) Yes, Don’t know (0) 5. Mouth and throat cancer—(0) No, (1) Yes, Don’t know (0) 6. Stroke—(0) No, (1) Yes, Don’t know (0) |
| Forgoing | In the last 30 days, have the warning labels stopped you from having a cigarette when you were about to smoke one?—(0) Never, (1) Once, (1) A few times, (1) Many times, or Don’t know (coded as missing) |
| Avoiding | In the last 30 days, have you made any effort to avoid looking at or thinking about the warning labels, such as covering them up, keeping them out of sight, using a cigarette case, avoiding certain warnings, or any other means?—No, Yes, or Don’t know (coded as missing) |
| Quit intention | Are you planning to quit smoking within the next 6 months?—(1) Very unlikely, (2) Unlikely, (3) Possibly, (4) Likely, (5) Very likely, or Don’t know (coded as missing) |
| Policy relevant outcomes (Wave 11) | |
| Quit attempts | Have you made any attempts (successful or not) to stop smoking in the last 12 months?—No, Yes |
| Smoking cessation | Smokers from Wave 10 who remained in the sample and who, in Wave 11, indicated to have quit smoking |
| Measures | |
|---|---|
| Control variables (Wave 10) | |
| Gender (n = 1038) | |
| Male (%) | 41.2 |
| Female (%) | 58.8 |
| Age (n = 1038) | |
| 15–24 (%) | 9.9 |
| 25–39 (%) | 20.4 |
| 40–45 (%) | 31.9 |
| 55+ (%) | 37.8 |
| Education (n = 1018) | |
| Low (%) | 24.3 |
| Moderate (%) | 44.1 |
| High (%) | 31.6 |
| Level of nicotine dependence (mean, SD) (n = 1010) | 2.06 (1.51) |
| Time in sample (mean, SD) (n = 1038) | 4.75 (3.24) |
| Smoking frequency (n = 1038) | |
| Daily (%) | 90 |
| Non-daily (%) | 10 |
| Policy specific variable (Wave 10) | |
| Health warning salience (mean, SD) (n = 1012) | 2.48 (1.09) |
| Psychosocial mediators (Wave 10) | |
| Attitude towards quitting (mean, SD) (n = 1018) | 4.04 (0.80) |
| Perceived social norms (n = 986) | 4.24 (0.81) |
| Self-efficacy (mean, SD) (n = 1008) | 2.28 (1.05) |
| Health worries (mean, SD) (n = 920) | 2.14 (0.76) |
| Knowledge (mean, SD) (n = 1038) | 3.89 (1.93) |
| Forgoing (n = 979) | |
| No (%) | 91.1 |
| Yes (%) | 8.9 |
| Avoiding (n = 967) | |
| No (%) | 79.7 |
| Yes (%) | 20.3 |
| Quit intention (mean, SD) (n = 1003) | 2.73 (1.22) |
| Policy relevant outcomes (Wave 11) | |
| Quit attempts (n = 898) | |
| No (%) | 72.9 |
| Yes (%) | 27.1 |
| Smoking cessation (n = 1023) | |
| No (%) | 90.0 |
| Yes (%) | 10.0 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Policy specific variable | ||||||||||
| 1. Health warning salience | ||||||||||
| Psychosocial mediators | ||||||||||
| 2. Attitude towards quitting | 0.165 *** | |||||||||
| 3. Perceived social norms | 0.182 *** | 0.498 *** | ||||||||
| 4. Self-efficacy | −0.025 | −0.084 ** | −0.184 *** | |||||||
| 5. Health worries | 0.350 *** | 0.368 *** | 0.219 *** | 0.041 | ||||||
| 6. Knowledge | 0.216 *** | 0.260 *** | 0.174 *** | 0.044 | 0.298 *** | |||||
| 7. Forgoing | 0.206 *** | 0.060 | −0.060 | 0.070 * | 0.191 *** | 0.027 | ||||
| 8. Avoiding | 0.163 *** | 0.048 | 0.070 * | −0.074 * | 0.166 *** | 0.002 | 0.166 *** | |||
| 9. Quit intention | 0.221 *** | 0.343 *** | 0.147 *** | 0.294 *** | 0.414 *** | 0.176 *** | 0.147 *** | 0.060 | ||
| Policy relevant outcomes | ||||||||||
| 10. Quit attempts | 0.040 | 0.164 *** | 0.140 *** | 0.113 ** | 0.217 *** | 0.119 *** | 0.040 | 0.031 | 0.373 *** | |
| 11. Smoking cessation | −0.015 | 0.096 ** | 0.076 * | 0.031 | 0.047 | 0.024 | −0.015 | −0.010 | 0.171 *** | 0.476 *** |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Policy specific variable | ||||||||||
| 1. Health warning salience | ||||||||||
| Psychosocial mediators | ||||||||||
| 2. Attitude towards quitting | 0.180 *** | |||||||||
| 3. Perceived social norms | 0.166 *** | |||||||||
| 4. Self-efficacy | 0.030 | |||||||||
| 5. Health worries | 0.301 *** | |||||||||
| 6. Knowledge | 0.155 *** | |||||||||
| 7. Forgoing | 0.396 *** | |||||||||
| 8. Avoiding | 0.192 ** | |||||||||
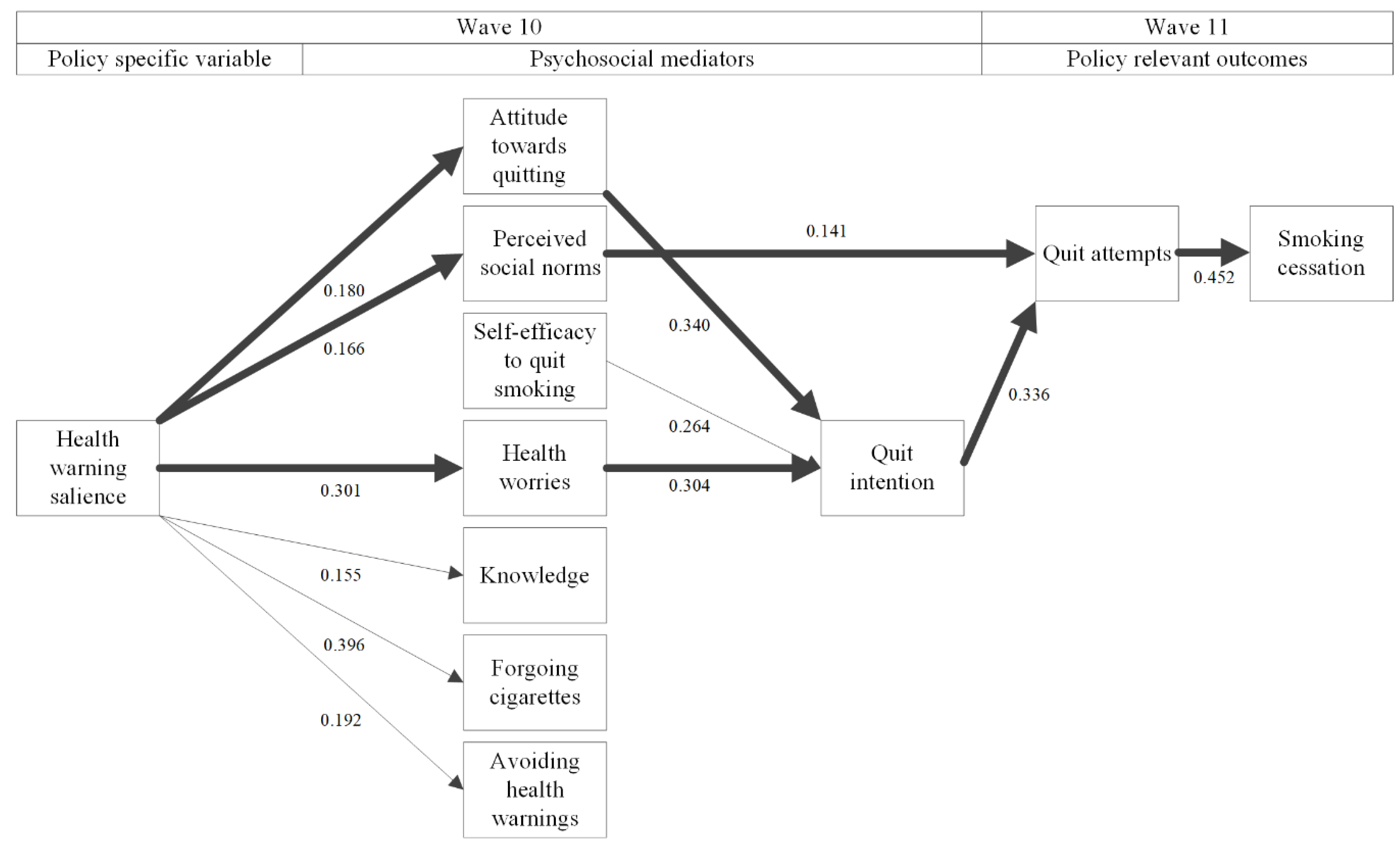
| 9. Quit intention | 0.042 | 0.340 *** | 0.016 | 0.264 *** | 0.304 *** | −0.070 | 0.172 | −0.070 | ||
| Policy relevant outcomes | ||||||||||
| 10. Quit attempts | −0.068 | −0.053 | 0.141 * | −0.030 | 0.046 | 0.044 | 0.008 | 0.010 | 0.336 ** | |
| 11. Smoking cessation | 0.046 | 0.027 | 0.030 | −0.087 | −0.083 | −0.044 | −0.067 | −0.029 | 0.036 | 0.452 * |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Policy specific variable | ||||||||||
| 1. Health warning salience | ||||||||||
| Psychosocial mediators | ||||||||||
| 2. Attitude towards quitting | 0.213 *** | |||||||||
| 3. Perceived social norms | 0.196 *** | |||||||||
| 4. Self-efficacy | 0.047 | |||||||||
| 5. Health worries | 0.308 *** | |||||||||
| 6. Knowledge | 0.191 *** | |||||||||
| 7. Forgoing | 0.235 *** | |||||||||
| 8. Avoiding | 0.146 *** | |||||||||
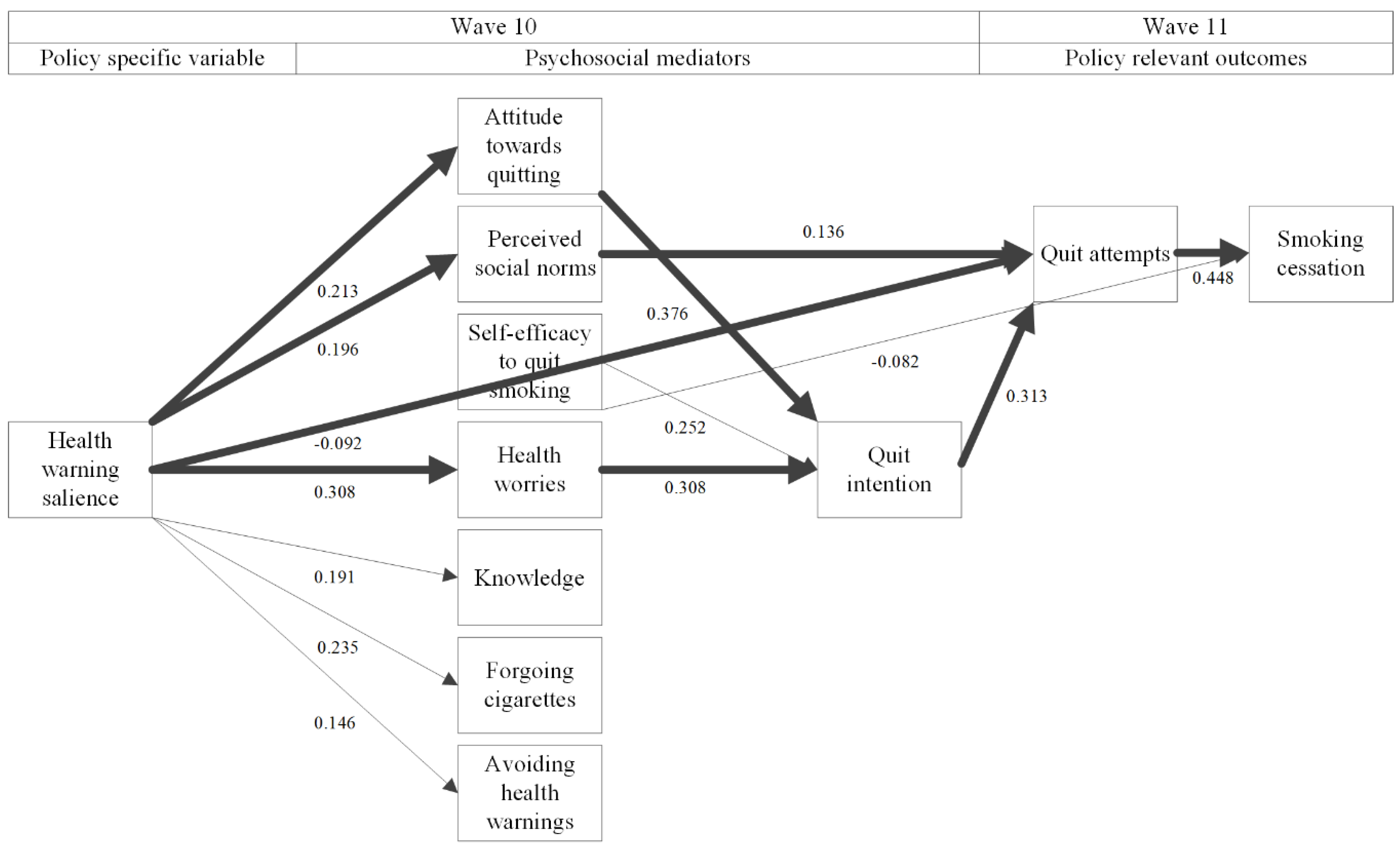
| 9. Quit intention | 0.063 | 0.376 *** | −0.048 | 0.252 *** | 0.308 *** | −0.040 | 0.059 | −0.012 | ||
| Policy relevant outcomes | ||||||||||
| 10. Quit attempts | −0.092 ** | −0.053 | 0.136 ** | −0.004 | 0.076 | 0.042 | 0.002 | 0.007 | 0.313 ** | |
| 11. Smoking cessation | 0.018 | 0.082 | 0.000 | −0.082 * | −0.087 | −0.043 | −0.041 | −0.017 | −0.006 | 0.448 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Mourik, D.-J.A.; Candel, M.J.J.M.; Nagelhout, G.E.; Willemsen, M.C.; Yong, H.-H.; van den Putte, B.; Fong, G.T.; de Vries, H. How the New European Union’s (Pictorial) Tobacco Health Warnings Influence Quit Attempts and Smoking Cessation: Findings from the 2016–2017 International Tobacco Control (ITC) Netherlands Surveys. Int. J. Environ. Res. Public Health 2019, 16, 4260. https://doi.org/10.3390/ijerph16214260
van Mourik D-JA, Candel MJJM, Nagelhout GE, Willemsen MC, Yong H-H, van den Putte B, Fong GT, de Vries H. How the New European Union’s (Pictorial) Tobacco Health Warnings Influence Quit Attempts and Smoking Cessation: Findings from the 2016–2017 International Tobacco Control (ITC) Netherlands Surveys. International Journal of Environmental Research and Public Health. 2019; 16(21):4260. https://doi.org/10.3390/ijerph16214260
Chicago/Turabian Stylevan Mourik, Dirk-Jan A., Math J. J. M. Candel, Gera E. Nagelhout, Marc C. Willemsen, Hua-Hie Yong, Bas van den Putte, Geoffrey T. Fong, and Hein de Vries. 2019. "How the New European Union’s (Pictorial) Tobacco Health Warnings Influence Quit Attempts and Smoking Cessation: Findings from the 2016–2017 International Tobacco Control (ITC) Netherlands Surveys" International Journal of Environmental Research and Public Health 16, no. 21: 4260. https://doi.org/10.3390/ijerph16214260