Using Patient-Reported Outcomes to Predict Revision Arthroplasty Following Femoral Neck Fracture: Enhancing the Value of Clinical Registries through Data Linkage

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Setting
2.2. Procedures
2.3. Data Linkage
2.4. Data Analysis
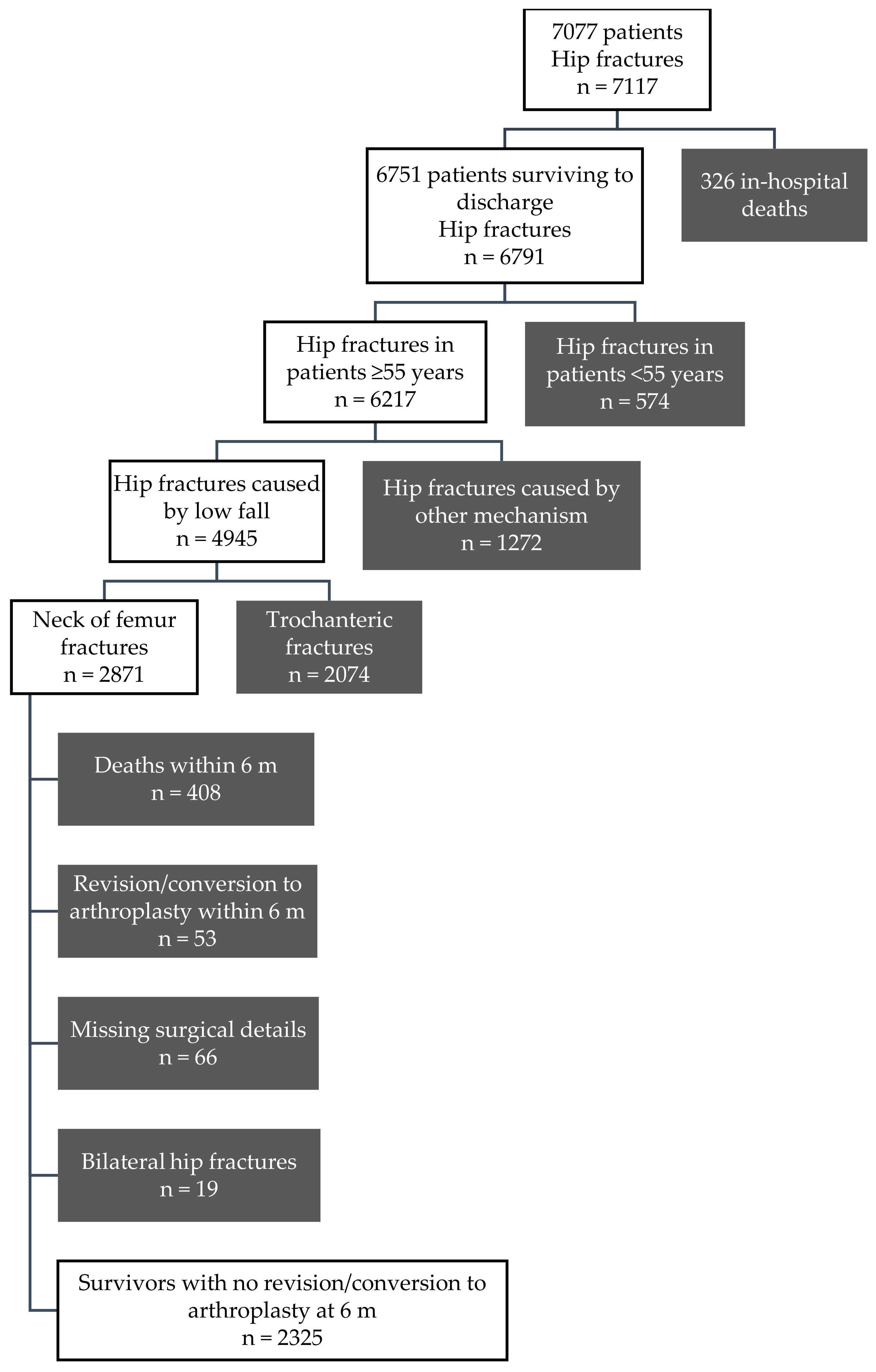
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Griffin, X.L.; Parsons, N.; Achten, J.; Fernandez, M.; Costa, M.L. Recovery of health-related quality of life in a United Kingdom hip fracture population. The Warwick Hip Trauma Evaluation—A prospective cohort study. Bone Jt. J. 2015, 97–B, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Paksima, N.; Koval, K.J.; Aharanoff, G.; Walsh, M.; Kubiak, E.N.; Zuckerman, J.D.; Egol, K.A. Predictors of mortality after hip fracture: A 10-year prospective study. Bull. NYU Hosp. Jt. Dis. 2008, 66, 111–117. [Google Scholar]
- Holt, G.; Smith, R.; Duncan, K.; Hutchison, J.D.; Reid, D. Changes in population demographics and the future incidence of hip fracture. Injury 2009, 40, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, L.E.; Culliford, D.; Monk, A.P.; Glyn-Jones, S.; Prieto-Alhambra, D.; Judge, A.; Cooper, C.; Carr, A.J.; Arden, N.K.; Beard, D.J.; et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: A population-based cohort study. Lancet 2017, 389, 1424–1430. [Google Scholar] [CrossRef]
- Jiang, J.; Yang, C.H.; Lin, Q.; Yun, X.D.; Xia, Y.Y. Does Arthroplasty Provide Better Outcomes Than Internal Fixation At Mid- and Long-term Followup? A Meta-analysis. Clin. Orthop. Relat. Res. 2015, 473, 2672–2679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, M.J.; Gurusamy, K. Internal fixation versus arthroplasty for intracapsular proximal femoral fractures in adults. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Conroy, J.L.; Whitehouse, S.L.; Graves, S.E.; Pratt, N.L.; Ryan, P.; Crawford, R.W. Risk Factors for Revision for Early Dislocation in Total Hip Arthroplasty. J. Arthroplast. 2008, 23, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Viberg, B.; Ryg, J.; Overgaard, S.; Lauritsen, J.; Ovesen, O. Low bone mineral density is not related to failure in femoral neck fracture patients treated with internal fixation. Acta Orthop. 2014, 85, 60–65. [Google Scholar] [CrossRef]
- Kim, C.; Nevitt, M.C.; Niu, J.; Clancy, M.M.; Lane, N.E.; Link, T.M.; Vlad, S.; Tolstykh, I.; Jungmann, P.M.; Felson, D.T.; et al. Association of hip pain with radiographic evidence of hip osteoarthritis: Diagnostic test study. BMJ 2015, 351. [Google Scholar] [CrossRef]
- Morshed, S.; Corrales, L.; Genant, H.; Miclau, T., 3rd. Outcome assessment in clinical trials of fracture-healing. J. Bone Jt. Surg. Am. 2008, 90 (Suppl. 1), 62–67. [Google Scholar] [CrossRef]
- Franklin, P.D.; Lewallen, D.; Bozic, K.; Hallstrom, B.; Jiranek, W.; Ayers, D.C. Implementation of patient-reported outcome measures in U.S. Total joint replacement registries: Rationale, status, and plans. J. Bone Jt. Surg. Am. 2014, 96 (Suppl. 1), 104–109. [Google Scholar] [CrossRef] [PubMed]
- Lacny, S.; Bohm, E.; Hawker, G.; Powell, J.; Marshall, D.A. Assessing the comparability of hip arthroplasty registries in order to improve the recording and monitoring of outcome. Bone Jt. J. 2016, 98-b, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Demographic Statistics. March 2017. Available online: http://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/3C252AE138902522CA2581A700158A3E/$File/final%203101%2022%20sep.pdf (accessed on 16 October 2017).
- VOTOR Steering Committee. Victorian Orthopaedic Trauma Outcomes Registry (VOTOR) Annual Report July 2015–June 2016. Available online: http://www.votor.org.au/node/13 (accessed on 18 February 2017).
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2017 Annual Report; AOA: Adelaide, Australia, 2017. [Google Scholar]
- National Centre for Classification in Health. International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM); National Centre for Classification in Health: Sydney, Australia, July 2010.
- Ekegren, C.L.; Edwards, E.R.; Page, R.; Hau, R.; de Steiger, R.; Bucknill, A.; Liew, S.; Oppy, A.; Gabbe, B.J. Twelve-month mortality and functional outcomes in hip fracture patients under 65 years of age. Injury 2016, 47, 2182–2188. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- National Centre for Classification in Health. The Australian Classification of Health Interventions (ACHI), 6th ed.; National Centre for Classification in Health, Faculty of Health Sciences, The University of Sydney: Sydney, Australia, 2008.
- Derrett, S.; Black, J.; Herbison, G. Outcome After Injury—A Systematic Literature Search of Studies Using the EQ-5D. J. Trauma 2009, 67, 883–890. [Google Scholar] [CrossRef]
- Gabbe, B.J.; McDermott, E.; Simpson, P.M.; Derrett, S.; Ameratunga, S.; Polinder, S.; Lyons, R.A.; Rivara, F.P.; Harrison, J.E. Level of agreement between patient-reported EQ-5D responses and EQ-5D responses mapped from the SF-12 in an injury population. Popul. Health Metr. 2015, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, J.D.W.; Lemeshow, S.; Sturdivant, R.X. Model-Building Strategies and Methods for Logistic Regression. In Applied Logistic Regression; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; Chapter 4; pp. 89–151. [Google Scholar] [CrossRef]
- Devane, P.; Horne, G.; Gehling, D.J. Oxford Hip Scores at 6 Months and 5 Years Are Associated With Total Hip Revision Within the Subsequent 2 Years. Clin. Orthop. 2013, 471, 3870–3874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothwell, A.G.; Hooper, G.J.; Hobbs, A.; Frampton, C.M. An analysis of the Oxford hip and knee scores and their relationship to early joint revision in the New Zealand Joint Registry. J. Bone Jt. Surg. Br. 2010, 92, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Britton, A.R.; Murray, D.W.; Bulstrode, C.J.; McPherson, K.; Denham, R.A. Pain levels after total hip replacement: Their use as endpoints for survival analysis. J. Bone Jt. Surg. Br. 1997, 79, 93–98. [Google Scholar] [CrossRef]
- Inacio, M.C.; Pratt, N.L.; Roughead, E.E.; Paxton, E.W.; Graves, S.E. Opioid use after total hip arthroplasty surgery is associated with revision surgery. BMC Musculoskelet. Disord. 2016, 17, 122. [Google Scholar] [CrossRef]
- The Swedish Hip Arthroplasty Register. The Swedish Hip Arthroplasty Register Annual Report 2015. Available online: https://registercentrum.blob.core.windows.net/shpr/r/Annual-Report-2015-H19dFINOW.pdf (accessed on 29 November 2017).
- Roder, C.; Bach, B.; Berry, D.J.; Eggli, S.; Langenhahn, R.; Busato, A. Obesity, age, sex, diagnosis, and fixation mode differently affect early cup failure in total hip arthroplasty: A matched case-control study of 4420 patients. J. Bone Jt. Surg. Am. 2010, 92, 1954–1963. [Google Scholar] [CrossRef]
- Sprague, S.; Schemitsch, E.H.; Swiontkowski, M.; Della Rocca, G.J.; Jeray, K.J.; Liew, S.; Slobogean, G.P.; Bzovsky, S.; Heels-Ansdell, D.; Zhou, Q.; et al. Factors Associated with Revision Surgery After Internal Fixation of Hip Fractures. J. Orthop. Trauma 2018, 32, 223–230. [Google Scholar] [CrossRef]
- Moerman, S.; Mathijssen, N.M.C.; Tuinebreijer, W.E.; Vochteloo, A.J.H.; Nelissen, R.G.H.H. Hemiarthroplasty and total hip arthroplasty in 30,830 patients with hip fractures: Data from the Dutch Arthroplasty Register on revision and risk factors for revision. Acta Orthop. 2018, 89, 509–514. [Google Scholar] [CrossRef]
- Rolfson, O.; Karrholm, J.; Dahlberg, L.E.; Garellick, G. Patient-reported outcomes in the Swedish Hip Arthroplasty Register: Results of a nationwide prospective observational study. J. Bone Jt. Surg. Br. 2011, 93, 867–875. [Google Scholar] [CrossRef]
- Ridgeway, S.; Wilson, J.; Charlet, A.; Kafatos, G.; Pearson, A.; Coello, R. Infection of the surgical site after arthroplasty of the hip. J. Bone Jt. Surg. Br. 2005, 87, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Heetveld, M.J.; Raaymakers, E.L.; van Eck-Smit, B.L.; van Walsum, A.D.; Luitse, J.S. Internal fixation for displaced fractures of the femoral neck. Does bone density affect clinical outcome? J. Bone Jt. Surg. Br. 2005, 87, 367–373. [Google Scholar] [CrossRef]
- Spangler, L.; Cummings, P.; Tencer, A.F.; Mueller, B.A.; Mock, C. Biomechanical factors and failure of transcervical hip fracture repair. Injury 2001, 32, 223–228. [Google Scholar] [CrossRef]
- Mathews, V.; Cabanela, M.E. Femoral Neck Nonunion Treatment. Clin. Orthop. Relat. Res. (1976–2007) 2004, 419, 57–64. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Patients with No Future Arthroplasty n (%) | Patients Undergoing Future Arthroplasty n (%) | p |
|---|---|---|---|
| Age group (years) | <0.001 | ||
| 55–64 | 134 (89.9) | 15 (10.1) | |
| 65–74 | 331 (94.0) | 21 (6.0) | |
| 75–84 | 857 (96.5) | 31 (3.5) | |
| 85+ | 926 (98.9) | 10 (1.1) | |
| Gender | 0.30 | ||
| Male | 618 (97.3) | 17 (2.7) | |
| Female | 1630 (96.5) | 60 (3.5) | |
| Pre-injury disability 1 | <0.001 | ||
| None | 769 (94.2) | 47 (5.8) | |
| Disability reported | 1257 (98.0) | 26 (2.0) | |
| Charlson Comorbidity Index at time of injury | <0.001 | ||
| 0 | 1165 (95.4) | 56 (4.6) | |
| ≥1 | 1083 (98.1) | 13 (1.9) | |
| Type index surgery | <0.001 | ||
| Cemented hemiarthroplasty | 1015 (98.5) | 16 (1.5) | |
| Cementless hemiarthroplasty | 345 (97.2) | 10 (2.8) | |
| Cemented total arthroplasty | 79 (95.2) | 4 (4.8) | |
| Cementless total arthroplasty | 67 (95.7) | 3 (4.3) | |
| Internal fixation | 742 (94.4) | 44 (5.6) | |
| Total | 2248 (96.7) | 77 (3.3) | - |
| Patient-Reported Outcomes | Patients with No Future Arthroplasty n (%) | Patients Undergoing Future Arthroplasty n (%) | p |
|---|---|---|---|
| Residence at 6 months post injury 1 | <0.001 | ||
| At home without additional care | 357 (94.0) | 23 (6.1) | |
| At home with additional care | 800 (95.1) | 41 (4.9) | |
| Nursing home/other | 890 (99.2) | 4 (0.8) | |
| Problems with mobility (EQ-5D) at 6 months post injury 2 | 0.28 | ||
| No | 257 (97.7) | 6 (2.3) | |
| Yes | 1592 (96.4) | 59 (3.6) | |
| Problems with personal care (EQ-5D) at 6 months post injury 3 | <0.01 | ||
| No | 628 (95.2) | 32 (4.9) | |
| Yes | 1177 (97.7) | 28 (2.3) | |
| Problems with usual activities (EQ-5D) at 6 months post injury 4 | 0.89 | ||
| No | 374 (96.6) | 13 (3.4) | |
| Yes | 1460 (96.5) | 53 (3.5) | |
| Pain and discomfort (EQ-5D) at 6 months post injury 5 | <0.001 | ||
| No | 842 (99.4) | 5 (0.6) | |
| Yes | 989 (94.0) | 63 (6.0) | |
| Anxiety (EQ-5D) at 6 months post injury 6 | 0.35 | ||
| No | 1043 (96.9) | 33 (3.1) | |
| Yes | 747 (96.1) | 30 (3.9) | |
| Total | 2248 (96.7) | 77 (3.3) | - |
| Covariate | HR | 95% CI | p |
|---|---|---|---|
| Age group (years) | <0.01 | ||
| 55–64 | 1.00 (ref) | ||
| 65–74 | 0.85 | 0.42, 1.73 | |
| 75–84 | 0.49 | 0.25, 0.95 | |
| 85+ | 0.22 | 0.09, 0.55 | |
| Pre-injury disability | <0.01 | ||
| None | 1.00 (ref) | ||
| Disability reported | 0.47 | 0.29, 0.78 | |
| Index surgery | 0.07 | ||
| Cemented hemiarthroplasty | 1.00 (ref) | ||
| Cementless hemiarthroplasty | 1.67 | 0.72, 3.84 | |
| Cemented total hip arthroplasty | 1.64 | 0.53, 5.01 | |
| Cementless total hip arthroplasty | 1.24 | 0.35, 4.35 | |
| Internal fixation | 2.41 | 1.31, 4.45 | |
| Pain and discomfort (EQ-5D) at 6 months post-injury | <0.001 | ||
| No | 1.00 (ref) | ||
| Yes | 9.50 | 3.81, 23.67 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekegren, C.L.; de Steiger, R.; Edwards, E.R.; Page, R.S.; Hau, R.; Liew, S.; Oppy, A.; Gabbe, B.J. Using Patient-Reported Outcomes to Predict Revision Arthroplasty Following Femoral Neck Fracture: Enhancing the Value of Clinical Registries through Data Linkage. Int. J. Environ. Res. Public Health 2019, 16, 1325. https://doi.org/10.3390/ijerph16081325
Ekegren CL, de Steiger R, Edwards ER, Page RS, Hau R, Liew S, Oppy A, Gabbe BJ. Using Patient-Reported Outcomes to Predict Revision Arthroplasty Following Femoral Neck Fracture: Enhancing the Value of Clinical Registries through Data Linkage. International Journal of Environmental Research and Public Health. 2019; 16(8):1325. https://doi.org/10.3390/ijerph16081325
Chicago/Turabian StyleEkegren, Christina L, Richard de Steiger, Elton R Edwards, Richard S Page, Raphael Hau, Susan Liew, Andrew Oppy, and Belinda J Gabbe. 2019. "Using Patient-Reported Outcomes to Predict Revision Arthroplasty Following Femoral Neck Fracture: Enhancing the Value of Clinical Registries through Data Linkage" International Journal of Environmental Research and Public Health 16, no. 8: 1325. https://doi.org/10.3390/ijerph16081325