Are Office-Based Workplace Interventions Designed to Reduce Sitting Time Cost-Effective Primary Prevention Measures for Cardiovascular Disease? A Systematic Review and Modelled Economic Evaluation


Abstract
:1. Introduction
2. Methods
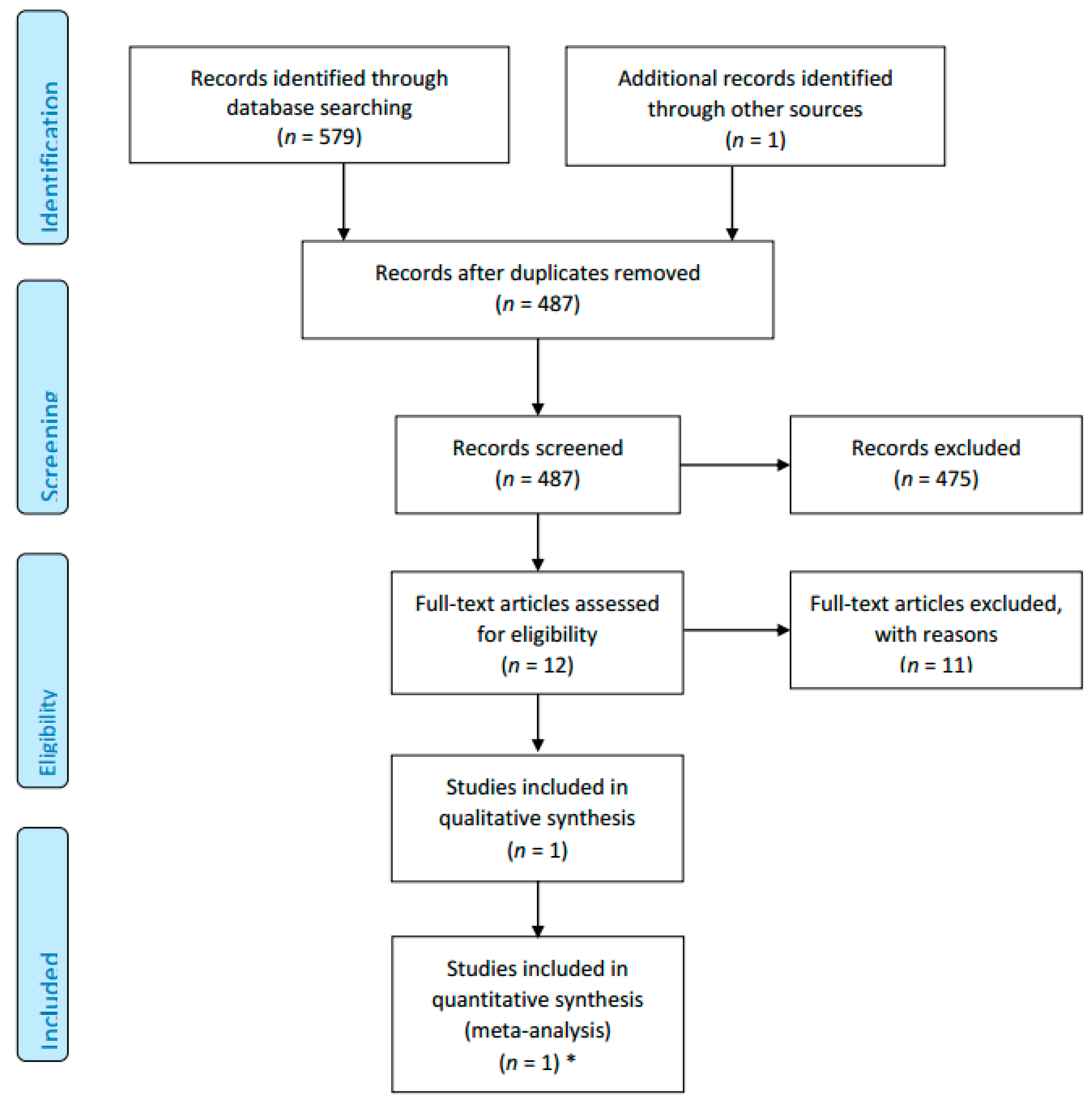
2.1. Systematic Review of Evidence
Search Strategy
2.2. Modelling the Long-Term CVD Outcome
2.2.1. Population
2.2.2. Model Structure
2.2.3. Outcome Measures
2.2.4. Disease Inputs
2.2.5. Costs
2.2.6. Utility Weights
2.2.7. Cost-Effectiveness Analysis
2.2.8. Ethical Statement
3. Results
3.1. Systematic Review of Workplace Interventions to Reduce Sitting Time
- Physical changes in workplace design and environment including changes in desks, chairs and workplace layout;
- Policies to modify the organisation of work including arranging walking meetings, encouraging breaks and completing sitting diaries;
- Provision of information and counselling including signs or prompts at the workplace, e-health interventions, distribution of leaflets and counselling.
3.2. Results of Modelling
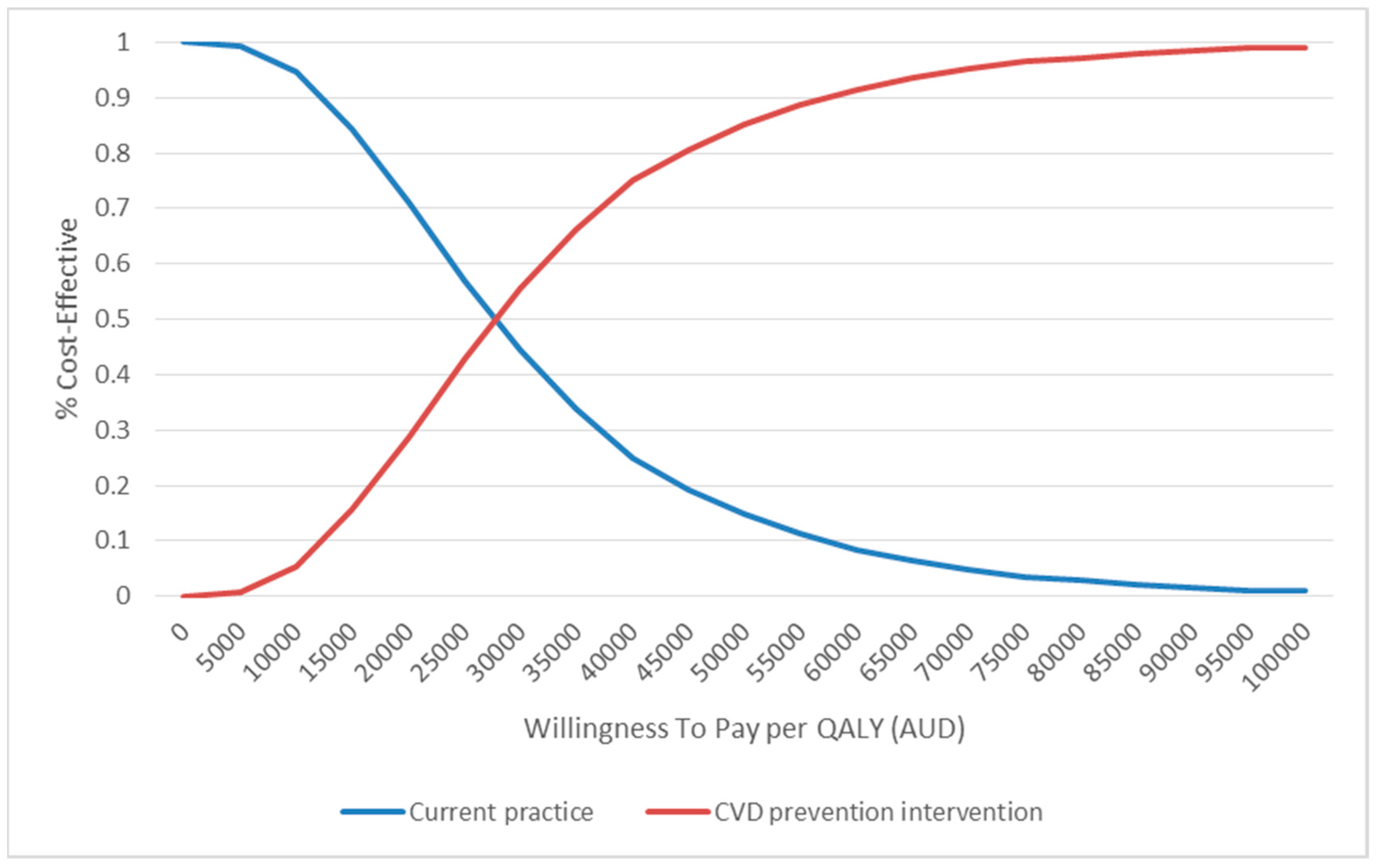
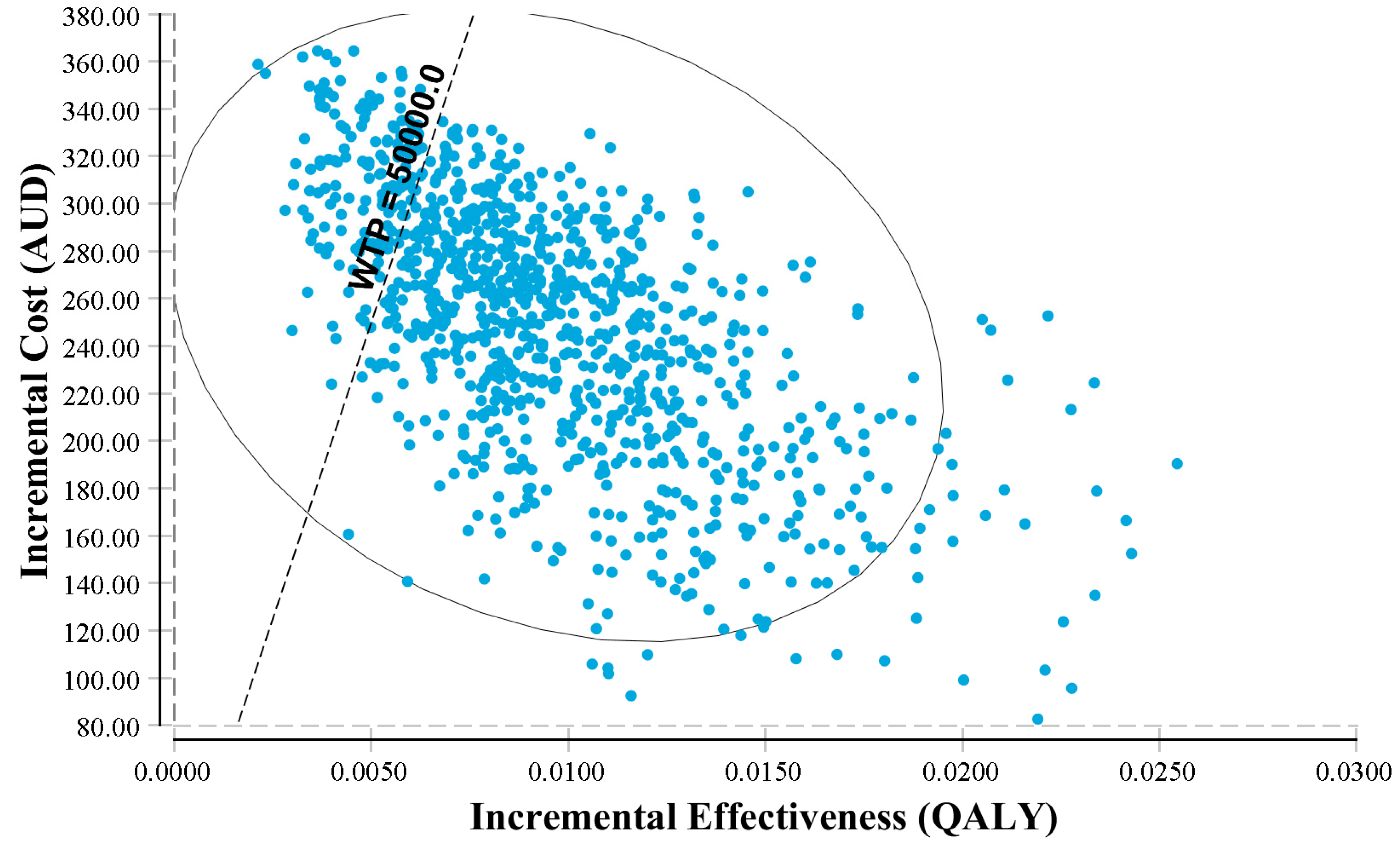
3.2.1. Cost-Effectiveness Analysis
3.2.2. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Search Strategies
Search Strategies:
Embase
| #1 sedentary |
| #2 ’sitting’/de |
| #3 ’seated posture’ |
| #4 seated NEAR/1 posture |
| #5 chair:ab,ti OR desk:ab,ti |
| #6 chair:ab,ti |
| #7 desk:ab,ti |
| #8 office AND inactiv* |
| #9 #1 OR #2 OR #4 OR #6 OR #7 OR #8 |
| #10 ’work’/de OR work |
| #11 work* |
| #12 ’occupation’/de OR occupation |
| #13 employe* |
| #14 #10 OR #12 OR #13 |
| #15 effect |
| #16 control |
| #17 evaluat* |
| #18 intervention* |
| #19 program |
| #20 compare |
| #21 #15 OR #16 OR #17 OR #18 OR #19 OR #20 |
| #22 #9 AND #14 AND #21 |
| #23 #22 AND [embase]/lim |
| #24 #23 AND [humans]/lim AND [embase]/lim |
Medline + PsyInfo (Via EBSCOhost Data Base)
| #1 (work[tw] OR works*[tw] OR work’*[tw] OR worka*[tw] OR worke*[tw] OR workg*[tw] OR worki*[tw] OR workl*[tw] OR |
| workp*[tw] OR occupation*[tw] OR employe*[tw]) |
| #2 (effect*[tw] OR control[tw] OR controls*[tw] OR controla*[tw] OR controle*[tw] OR controli*[tw] OR controll*[tw] OR evaluat*[tw] OR intervention*[tw] OR program*[tw] OR compare*[tw]) |
| #3 (sedentary OR sitting) OR seated posture OR chair[tiab] OR desk[tiab] OR (office AND inactiv*) |
| #4 (animals [mh] NOT humans [mh]) |
| #5 #1 AND #2 AND #3 NOT #4 |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters in the Model | Value Used in the Model | Source |
|---|---|---|
| Cost | ||
| Intervention | $431 | Gao et al., 2018 [51] |
| Incident stroke | $23,581 | IHPA * |
| Prevalent stroke | $3201 | Lim et al., 2005 |
| Incident CHD | $17,863 | IHPA * |
| Prevalent CHD | $4539 | Lim et al., 2005 |
| Utility weight | ||
| CHD | 0.86 | Cobiac et al., 2012 [26] |
| Stroke | 0.76 | Cobiac et al., 2012 [26] |
| Zhu 2018 | ||
|---|---|---|
| Methods | Cluster-random allocation (quasi-experimental) Unblinded Study duration: 18 months Dropout: 0% (100% retention) Location: Two units of a university, located in different buildings in the US Recruitment: Employees in each worksite were invited to participate via email lists. Participants signed consent form. | |
| Participants | Population: full time office workers (18–65 years old) Intervention group: 24 participants Control group: 12 participants Demographics: Mean age: 39.1 (SD 11.3); female 70.8%. | |
| Interventions | Duration of intervention: 4 months Intervention: Each participants received a sit-stand workstation at their primary work location. Three additional treadmill workstations were installed in common areas. E-Newsletters for social support and maintaining progress were sent to all staffs. Control: Staffs received newsletter as in intervention arm but no environmental changes were made. | |
| Outcomes | Outcome name, measurement time/tool (units of measurement)
| |
| Notes | This study was funded in part by the Virginia G. Piper Charitable Trust and the Steelcase Corporation. First author is supported by the Fundamental Research Funds for the Central Universities in China (GK201603128). Other authors are supported by the National Institute of Health (R01CA198971). | |
| Risk of bias | ||
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Randomisation was not done as participants in intervention and control groups were selected from different location of one workplace. |
| Allocation concealment (selection bias) | High risk | Intervention and control groups were selected from two separate locations. However no information on allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Virtually no attrition |
| Selective reporting (reporting bias) | Low risk | All outcomes mentioned in the method section were reported. Study protocol was not available. |
| Baseline comparability/imbalance | Low risk | No significant difference between groups at baseline was detected. |
| Validity of outcome measure | Low risk | All questionaries used were validated and relevant to China context. But physical activity and sedentary time were measured by accelerators. |
References
- Australian Institute of Health and Welfare. Cardiovascular Disease: Australian Facts 2011; Cardiovascular Disease Series; Cat. No. CVD 53; AIHW: Canberra, Australia, 2011.
- Waters, A.M.; Trinh, L.; Chau, T.; Bourchier, M.; Moon, L. Latest statistics on cardiovascular disease in Australia. Clin. Exp. Pharmacol. Physiol. 2013, 40, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Heart, Stroke and Vascular Diseases—Australian Facts 2004; Cardiovascular Disease Series No. 22; AIHW Cat. No. CVD 27; AIHW and National Heart Foundation of Australia: Canberra, Australia, 2004.
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Rev. Esp. Cardiol. (Engl. Ed.) 2016, 69, 939. [Google Scholar] [PubMed] [Green Version]
- National Vascular Disease Prevention Alliance, Guidelines for the Management of Absolute Cardiovascular Disease Risk. 2012. Available online: https://www.heartfoundation.org.au/images/uploads/publications/Absolute-CVD-Risk-Full-Guidelines.pdf (accessed on 26 July 2018).
- World Health Organization. Prevention of Cardiovascular Disease Guidelines for Assessment and Management of Cardiovascular Risk. 2007. Available online: http://www.who.int/cardiovascular_diseases/guidelines/Full%20text.pdf (accessed on 26 November 2018).
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Sarma, A.V.; Gordon, P.M. Sitting time and all-cause mortality risk. Arch. Intern. Med. 2012, 172, 1270–1272. [Google Scholar] [CrossRef] [PubMed]
- Van der Ploeg, H.P.; Chey, T.; Korda, R.J.; Banks, E.; Bauman, A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch. Intern. Med. 2012, 172, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Owen, N.; Biddle, S.J.; Dunstan, D.W. Managing sedentary behavior to reduce the risk of diabetes and cardiovascular disease. Curr. Diab. Rep. 2014, 14, 522. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.; Straker, L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health 2013, 13, 296. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Labor Statistics. Employment by Major Occupational Group, 2008 and Projected 2018; U.S. Department of Labor: Washington, DC, USA, 2010.
- Neuhaus, M.; Healy, G.N.; Fjeldsoe, B.S.; Lawler, S.; Owen, N.; Dunstan, D.W.; LaMontagne, A.D.; Eakin, E.G. Iterative development of Stand Up Australia: A multi-component intervention to reduce workplace sitting. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Van der Ploeg, H.P.; Chey, T.; Ding, D.; Chau, J.Y.; Stamatakis, E.; Bauman, A.E. Standing time and all-cause mortality in a large cohort of Australian adults. Prev. Med. 2014, 69, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting Time and Mortality from All Causes, Cardiovascular Disease, and Cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamatakis, E.; Rogers, K.; Ding, D.; Berrigan, D.; Hamer, M.; Chau, J.; Bauman, A. Replacing sedentary time with standing, physical activity, and sleeping: Associations with all-cause mortality in a cohort of 201,129 Australian adults. J. Sci. Med. Sport 2014, 18, e40. [Google Scholar] [CrossRef]
- Healy, G.N.; Eakin, E.G.; Owen, N.; Lamontagne, A.D.; Moodie, M.; Winkler, E.A.; Fjeldsoe, B.S.; Wiesner, G.; Willenberg, L.; Dunstan, D.W. A Cluster Randomized Controlled Trial to Reduce Office Workers’ Sitting Time: Effect on Activity Outcomes. Med. Sci. Sports Exerc. 2016, 48, 1787–1797. [Google Scholar] [CrossRef] [PubMed]
- Edwardson, C.L.; Yates, T.; Biddle, S.J.H.; Davies, M.J.; Dunstan, D.W.; Esliger, D.W.; Gray, L.J.; Jackson, B.; O’Connell, S.E.; Waheed, G.; et al. Effectiveness of the Stand More AT (SMArT) Work intervention: Cluster randomised controlled trial. BMJ 2018, 363, k3870. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Winkler, E.A.H.; Eakin, E.G.; Owen, N.; Lamontagne, A.D.; Moodie, M.; Dunstan, D.W. A Cluster RCT to Reduce Workers’ Sitting Time: Impact on Cardiometabolic Biomarkers. Med. Sci. Sports Exerc. 2017, 49, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Ijaz, S.; Kukkonen-Harjula, K.T.; Kumar, S.; Nwankwo, C.P. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2015, 1, CD010912. [Google Scholar] [PubMed] [Green Version]
- Cochrane Library. Assessing Risk of Bias in Included Studies. Cochrane Handbook. Available online: https://methods.cochrane.org/bias/assessing-risk-bias-included-studies (accessed on 26 November 2018).
- Australian Bureau of Statistics. 3101.0-Australian Demographic Statistics, December 2017. 2018. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3101.0Dec%202017?OpenDocument (accessed on 26 November 2018).
- Australian Bureau of Statistics. 4364.0.55.001-National Health Survey: First Results, 2014–15. 2015. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0012014-15?OpenDocument (accessed on 26 November 2018).
- Cobiac, L.J.; Magnus, A.; Lim, S.; Barendregt, J.J.; Carter, R.; Vos, T. Which interventions offer best value for money in primary prevention of cardiovascular disease? PLoS ONE 2012, 7, e41842. [Google Scholar] [CrossRef] [PubMed]
- Cobiac, L.J.; Vos, T.; Veerman, J.L. Cost-effectiveness of interventions to reduce dietary salt intake. Heart 2010, 96, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, N.; Blakely, T.; Cobiac, L.J.; Cleghorn, C.L.; Wilson, N. The health gains and cost savings of dietary salt reduction interventions, with equity and age distributional aspects. BMC Public Health 2016, 16, 423. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Types of Cardiovascular Diseases. Available online: http://www.who.int/cardiovascular_diseases/en/cvd_atlas_01_types.pdf (accessed on 26 November 2018).
- Universiyt of Colorado Hospital. CU Sports Medicine, Estimating Energy Expenditure. Available online: http://www.ucdenver.edu/academics/colleges/medicine/sportsmed/cusm_patient_resources/Documents/Estimating%20Energy%20Expenditure.pdf (accessed on 26 November 2018).
- Cobiac, L.J.; Vos, T.; Barendregt, J.J. Cost-effectiveness of interventions to promote physical activity: A modelling study. PLoS Med. 2009, 6, e1000110. [Google Scholar] [CrossRef] [PubMed]
- Begg, S.J.; Vos, T.; Barker, B.; Stanley, L.; Lopez, A.D. Burden of disease and injury in Australia in the new millennium: Measuring health loss from diseases, injuries and risk factors. Med. J. Aust. 2008, 188, 36–40. [Google Scholar] [PubMed]
- Mora, S.; Cook, N.; Buring, J.E.; Ridker, P.M.; Lee, I.M. Physical activity and reduced risk of cardiovascular events: Potential mediating mechanisms. Circulation 2007, 116, 2110–2118. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.; Siegel, J.; Russell, L.; Weinstein, M.C. Cost Effectiveness in Health and Medicine; Oxford University Press: New York, NY, USA, 1996. [Google Scholar]
- Shih, S.T.; Carter, R.; Heward, S.; Sinclair, C. Economic evaluation of future skin cancer prevention in Australia. Prev. Med. 2017, 99, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Australia Bureau of Statistics. Physical Activity in Australia 2007-08. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/4835.0.55.001 (accessed on 26 November 2018).
- Zhu, W.; Gutierrez, M.; Toledo, M.J.; Mullane, S.; Stella, A.P.; Diemar, R.; Buman, K.F.; Buman, M.P. Long-term effects of sit-stand workstations on workplace sitting: A natural experiment. J. Sci. Med. Sport 2018, 21, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.P.; Hong, O.; Lin, C.C.; Lu, S.H.; Chen, M.M.; Lee, K.C. A “Sit Less, Walk More” workplace intervention for office workers: Long-term efficacy of a quasi-experimental study. J. Occup. Environ. Med. 2018, 60, e290–e299. [Google Scholar] [CrossRef] [PubMed]
- Young, D.R.; Hivert, M.F.; Alhassan, S.; Camhi, S.M.; Ferguson, J.F.; Katzmarzyk, P.T.; Lewis, C.E.; Owen, N.; Perry, C.K.; Siddique, J.; et al. Sedentary behavior and cardiovascular morbidity and mortality: A science advisory from the American Heart Association. Circulation 2016, 134, e262–e279. [Google Scholar] [CrossRef] [PubMed]
- Department of Health Australia. Australia’s Physical Activity and Sedentary Behaviour Guidelines. 2017. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines#apaadult (accessed on 26 July 2018).
- Canadian Society for Exercise Physiology. Canadian Physical Activity, and Sedentary Behaviour Guidelines; Canadian Society for Exercise Physiology: Ottawa, ON, Canada, 2012. [Google Scholar]
- UK Department of Health, Physical Activity, Health Improvement and Protection. Start Active, Stay Active: A Report on Physical Activity for Health from the Four Home Countries’ Chief Medical Officers; DH: London, UK. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/216370/dh_128210.pdf (accessed on 26 November 2018).
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.A.; Ortiz, M.; Calcino, G. Persistence with antihypertensive medication: Australia-wide experience, 2004–2006. Med. J. Aust. 2008, 188, 224–227. [Google Scholar] [PubMed]
- Plotnikoff, R.; Karunamuni, N. Reducing sitting time: The new workplace health priority. Arch. Environ. Occup. Health 2012, 67, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Bellettiere, J.; Winkler, E.A.H.; Chastin, S.F.M.; Kerr, J.; Owen, N.; Dunstan, D.W.; Healy, G.N. Associations of sitting accumulation patterns with cardio-metabolic risk biomarkers in Australian adults. PLoS ONE 2017, 12, e0180119. [Google Scholar] [CrossRef] [PubMed]
- Bey, L.; Hamilton, M.T. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: A molecular reason to maintain daily low-intensity activity. J. Physiol. 2003, 551 Pt 2, 673–682. [Google Scholar] [CrossRef]
- Brocklebank, L.A.; Falconer, C.L.; Page, A.S.; Perry, R.; Cooper, A.R. Accelerometer-measured sedentary time and cardiometabolic biomarkers: A systematic review. Prev. Med. 2015, 76, 92–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buman, M.P.; Winkler, E.A.; Kurka, J.M.; Hekler, E.B.; Baldwin, C.M.; Owen, N.; Ainsworth, B.E.; Healy, G.N.; Gardiner, P.A. Reallocating time to sleep, sedentary behaviors, or active behaviors: Associations with cardiovascular disease risk biomarkers, NHANES 2005–2006. Am. J. Epidemiol. 2014, 179, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Flego, A.; Dunstan, D.W.; Winkler, E.A.; Healy, G.N.; Eakin, E.G.; Willenberg, L.; Owen, N.; LaMontagne, A.D.; Lal, A.; et al. Economic evaluation of a randomized controlled trial of an intervention to reduce office workers’ sitting time: The “Stand Up Victoria” trial. Scand. J. Work Environ. Health 2018, 44, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Coenen, P.; Howie, E.; Lee, J.; Williamson, A.; Straker, L. A detailed description of the short-term musculoskeletal and cognitive effects of prolonged standing for office computer work. Ergonomics 2018, 61, 877–890. [Google Scholar] [CrossRef] [PubMed]
- 2018 Physical Activity Guidelines Advisory Committee, Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- National Hospital Cost Data Collection, Independent hospital Pricing Authority (IHPA). Available online: https://www.ihpa.gov.au/what-we-do/nhcdc (accessed on 26 November 2018).



| Intervention | Comparator | Changes in Standing Time (Min/Day, 95% CI) | p-Value |
|---|---|---|---|
| Sit-stand desk with or without information and counselling | Sit-desk | 40.85 (26.18, 59.42) * | p < 0.001 |
| Information, feedback and/or reminder | No intervention | 10.24 (−17.17, 37.65) | p > 0.05 |
| Prompts plus information | Information alone | 32.40 (−6.81, 71.61) | p > 0.05 |
| Computer prompts to step | Computer prompts to stand | −11.9 (−15.33, −8.47) | p > 0.05 |
| Activity tracker combined with organisational support | Organisation support | 3.40 (−19.80, 26.60) | p > 0.05 |
| Groups | Base Case Results | |||
|---|---|---|---|---|
| Cost | QALY | ICER | ||
| Intervention | $6820 | 23.280 | - | |
| Control | $6524 | 23.273 | - | |
| Difference | $170 | 0.007 | $43,825/QALY | |
| Probabilistic sensitivity analyses | ||||
| QALY (mean, 95% CI) | Cost (mean, 95% CI) | |||
| Intervention | 23.255 (23.104, 23.360) | $6342 ($5545, $7232) | ||
| Control | 23.245 (23.089, 23.354) | $6093 ($5288, $6998) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, L.; Nguyen, P.; Dunstan, D.; Moodie, M. Are Office-Based Workplace Interventions Designed to Reduce Sitting Time Cost-Effective Primary Prevention Measures for Cardiovascular Disease? A Systematic Review and Modelled Economic Evaluation. Int. J. Environ. Res. Public Health 2019, 16, 834. https://doi.org/10.3390/ijerph16050834
Gao L, Nguyen P, Dunstan D, Moodie M. Are Office-Based Workplace Interventions Designed to Reduce Sitting Time Cost-Effective Primary Prevention Measures for Cardiovascular Disease? A Systematic Review and Modelled Economic Evaluation. International Journal of Environmental Research and Public Health. 2019; 16(5):834. https://doi.org/10.3390/ijerph16050834
Chicago/Turabian StyleGao, Lan, Phuong Nguyen, David Dunstan, and Marjory Moodie. 2019. "Are Office-Based Workplace Interventions Designed to Reduce Sitting Time Cost-Effective Primary Prevention Measures for Cardiovascular Disease? A Systematic Review and Modelled Economic Evaluation" International Journal of Environmental Research and Public Health 16, no. 5: 834. https://doi.org/10.3390/ijerph16050834