Understanding Health Promotion Policy Processes: A Study of the Government Adoption of the Achievement Program in Victoria, Australia


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Scope
2.2. Research Setting
2.3. Data Collection
2.3.1. Semi-Structured Interviews
2.3.2. Documents
2.4. Data Analysis
Causal Loop Diagrams (CLD)
2.5. Data Reporting
2.6. Ethics Approval
3. Results
3.1. Advocacy Coalition Framework Analysis
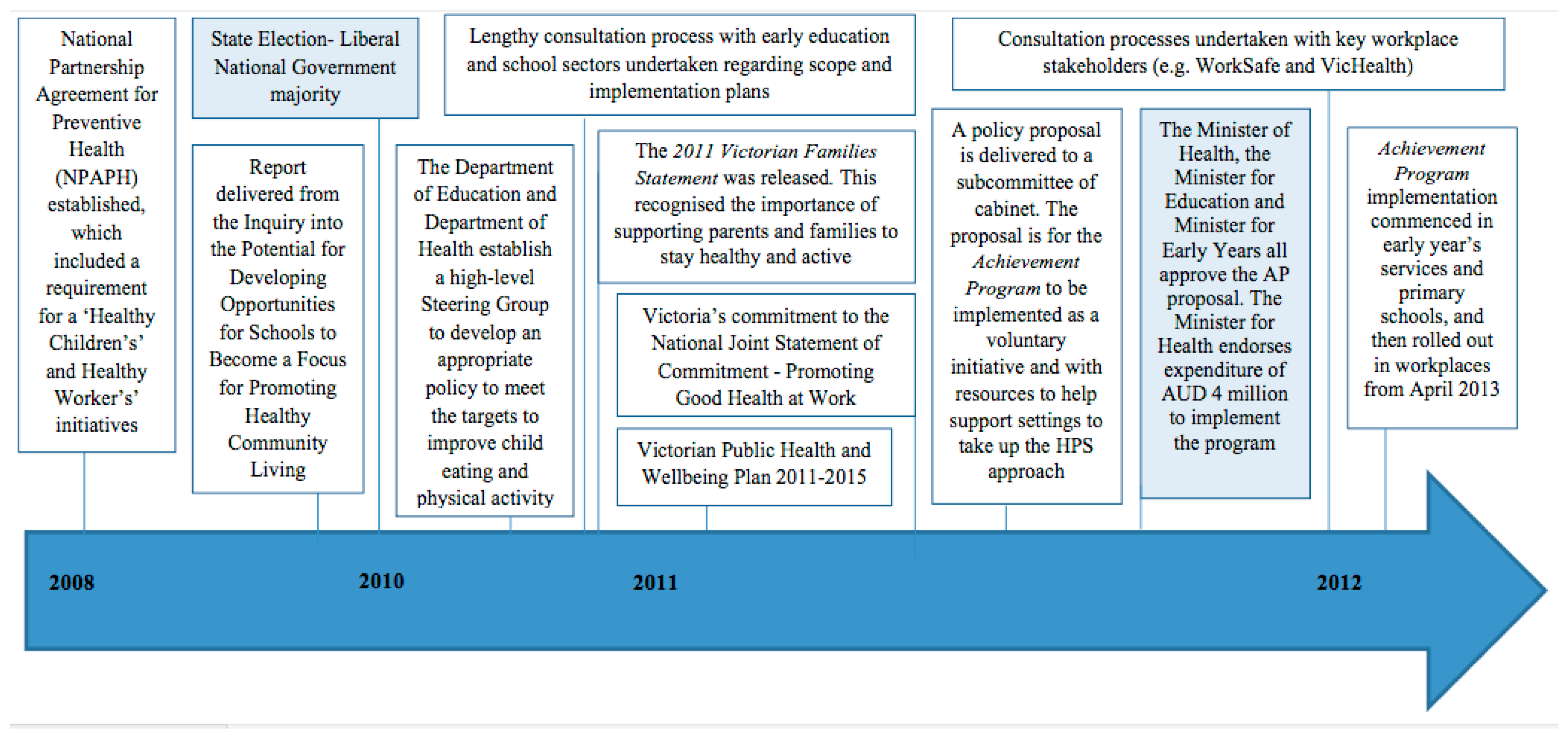
3.1.1. External Subsystem Events
“It [the emphasis of the need for the policy] was all around the National Partnership Agreement and we had a mandate and money to do something…and we had targets [that] we had to meet from the Commonwealth so there was an imperative for us to do something.”(Senior Policy Maker 1)
“There were some incredibly tight timeframes around getting something up and running because KGFYL was ceasing so there was, from a department and ministerial perspective, there was a risk in having any great length of delay in going from the KGFYL”(Policy Maker 1)
3.1.2. Coalition Opportunity Structures
“…What we foresaw before we engaged [a stakeholder organisation] was that they could see the Achievement Program as competition and we didn’t want that to be the case…we wanted to engage them right from the beginning to talk about how we weren’t trying to be in competition with what they were doing”(Policy Maker 4)
3.2. Action Arenas and Patterns of Interaction (Institutional Analysis and Development Framework)
“So the network and the distribution of power; that original steering group really only had two representatives from the Department of Health and about eight from Department of Education, so we deliberately sought to shift some of that power to Education as a strategy to engage them, to give them a little bit more power and control over the direction to inform it right from the beginning.”(Policy Maker 2)
3.3. Institutional Rules and Procedures
3.3.1. Advocacy Coalitions
3.3.2. Belief Systems
3.4. Core Beliefs
“So certainly from Worksafe’s point of view, something that came through very strongly was that anything in this [policy] space could only be voluntary.”(Policy Maker 1)
3.5. Policy Beliefs
“I do also think that the Secretary at the time understood that agenda—understood the prevention agenda and was also highly supportive of it.”(Senior Policy Maker 2)
“…We were under a Liberal government, so we kept emphasising that the state has signed up to this, we have to do it, the money’s coming. [So that there was] no opportunity to shut this down, because we didn’t know what the Liberals would think. As it turned out we had a wonderful Minister who totally understood public health so it wasn’t really an issue but you just never know because sometimes the values don’t align.”(Senior Policy Maker 1)
Policy Brokers
“[A Senior Public Health Advisor] did a lot of the heavy lifting with a lot of those individual groups, which was not always straightforward. There was a bit of push back, [but] they were, in the end, actually very supportive [of the Achievement Program].”(Senior Policy Maker 2)
3.6. Multiple Streams Theory Analysis
3.6.1. Problem Stream
3.6.2. Politics Stream
3.7. Political Interests
“[The AP] delivered lots of good things for them [the Minister for Health], because there were lots of good news stories lots of photo ops [opportunities], lots of chances to go out and meet and greet.”(Senior Policy Maker 1)
“…The political cycle always has a role…so at that stage [with the change in government] you are usually looking for something new…we couldn’t have [KGFYL] anymore.”(Senior Policy Maker 2)
“We were very fortunate with the factions within the government. When we were developing the AP, the Health Minister also had a good relationship with the Early Childhood Minister so there was a connection which helped.”(Senior Policy Maker 1)
Policy Stream
“…It is not a high cost initiative and, given the reach, it was a reasonably easy thing I think for the government to agree to…”(Policy Director 1)
“I would say the complication we had was working out the delivery, [with] the DHHS not being a delivery body. The decisions around, who do we fund to do this? I think that’s where some of the…well, kind of turf conflict [between public health organisations who seek funding to implement the health promotion programs] came out a little bit.”(Policy Maker 1)
3.8. Framing
“[When one of the policy entrepreneurs] spoke to the Secretary about this approach, [they] would be talking about that the hospital system has quality measures, [and that] we are trying to do the same thing for prevention. So it was about creating the match between where [the Secretary] wanted to go and what this might deliver for [them].”(Senior Policy Maker 2)
“…It was about really articulating how the Achievement Program would help them [early childcare settings] meet the National Quality Standards that they had to meet and how it could support that for schools. It was about trying to line up the process and then demonstrate to schools how the quality improvement process that they went through with the Achievement Program was no different to the process that they were required to do otherwise by Department of Education. For workplaces, it was about demonstrating more the business case to them around the benefits, but these were all factors that enabled us to get the right kind of support to support its development.”(Policy Maker 2)
3.8.1. Policy Windows and Entrepreneurs
“…I give [one particular policy entrepreneur] an enormous credit for a lot because [they] really did drive it. [They] were a tough taskmaster but a pretty strong captain of the ship…that strong leadership [was] right up front.”(Senior Policy Maker 2)
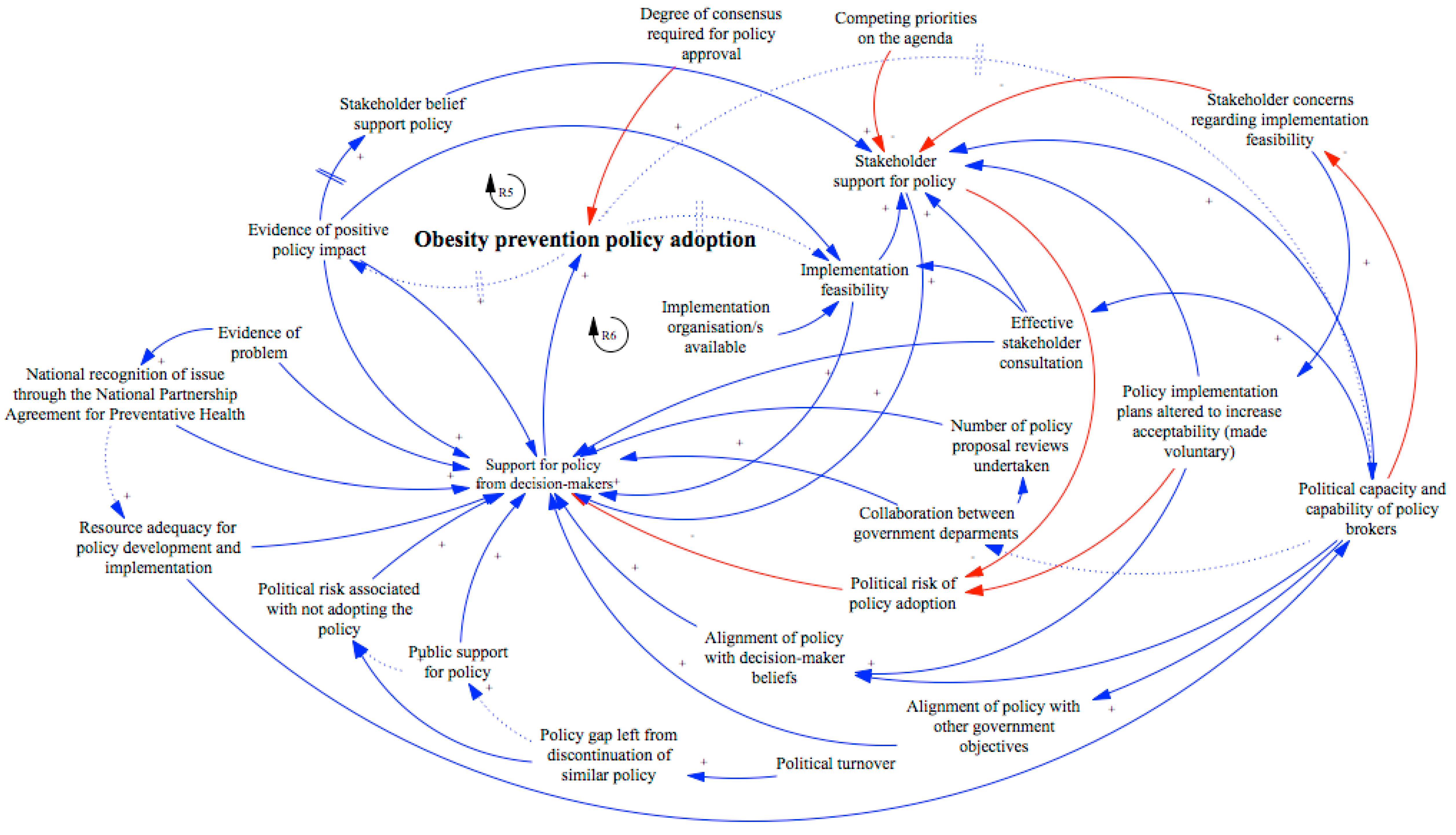
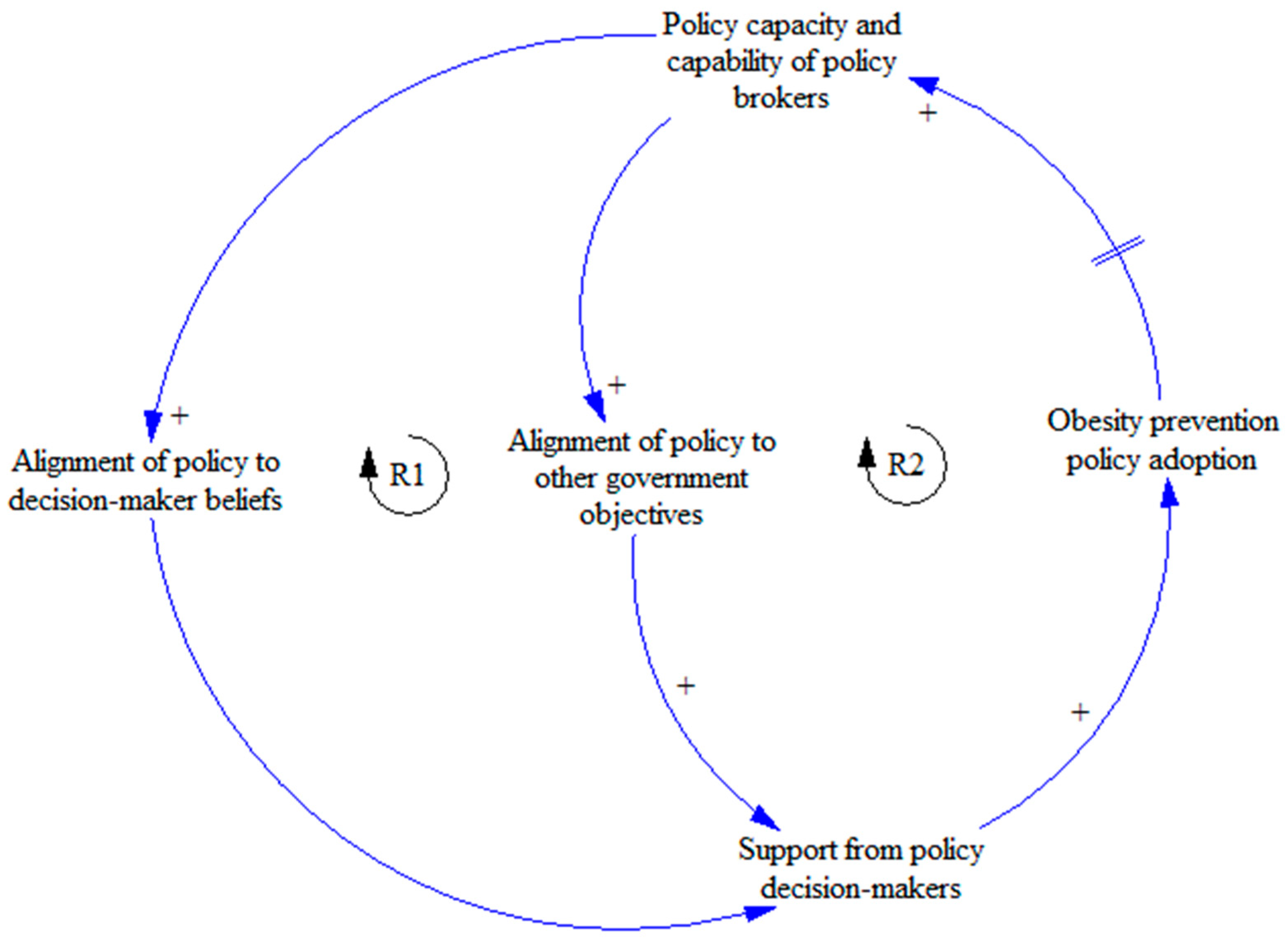
3.8.2. The Achievement Program Policy System
4. Discussion
4.1. Stakeholder Resistance
4.2. Beliefs
4.3. Framing
4.4. Institutional Factors
4.5. Complexity of the Policy Process
- Explicitly consider the policy implementation requirements (e.g., feasibility issues) at an early stage of the policy development process in order to identify potential risks of policy adoption and inform the development of risk management strategies (e.g., reframing policy solutions, consultations and negotiations strategies);
- Advocate the establishment of organisation structures that support collaboration and open, transparent policy development processes to assist in creating fairer opportunities for a broad range of external stakeholders to contribute to policy development. This is particularly important given the increasingly noted efforts of the food industry to influence policy makers, and the privileged access to decision makers that they often enjoy [81,82];
- Alter policy framing to align with broader government objectives, dominant belief systems and to minimise political risk (e.g., resistance from stakeholders).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- World Health Organization WHO. Global Status Report on Noncommunicable Diseases 2010; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.K.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 13, 2400–2409. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.T.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Promoting Health Through Schools; Report of a WHO Expert Committee on Comprehensive School Health Education and Promotion; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity prevention and the Health promoting Schools framework: Essential components and barriers to success. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Komro, K.; Murphy, S.; Magnus, D.; Waters, E.; Gibbs, L.; Campbell, R. The Health Promoting Schools Framework: Known Unknowns and an Agenda for Future Research. Health Educ. Behav. 2016, 44, 463–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Human Services (DHHS). What Is the Achievement Program? Available online: http://www.achievementprogram.health.vic.gov.au/health-professionals/what-it-is (accessed on 16 May 2017).
- Clarke, B.; Swinburn, B.; Sacks, G. The application of theories of the policy process to obesity prevention: A systematic review and meta-synthesis. BMC. Pub. Health 2016, 16, 1084. [Google Scholar] [CrossRef] [PubMed]
- Crammond, B.; Van, C.; Allender, S.; Peeters, A.; Lawrence, M.; Sacks, G.; Mavoa, H.; Swinburn, B.A.; Loff, B. The possibility of regulating for obesity prevention—Understanding regulation in the Commonwealth Government. Obes. Rev. 2013, 14, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Waqa, G.; Mavoa, H.; Snowdon, W.; Moodie, M.; Schultz, J.; McCabe, M.; Kremer, P.; Swinburn, B. Knowledge brokering between researchers and policymakers in Fiji to develop policies to reduce obesity: A process evaluation. Implement. Sci. 2013, 8, 74. [Google Scholar] [CrossRef] [PubMed]
- Shill, J.; Mavoa, H.; Allender, S.; Lawrence, M.; Sacks, G.; Peeters, A.; Crammond, B.; Swinburn, B. Government regulation to promote healthy food environments: A view from inside state governments. Obes. Rev. 2012, 13, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Cheadle, A.; Podrabsky, M.; Quinn, E.; MacDougall, E.; Cechovic, K.; Kovacs, T.; Lane, C.; Sitaker, M.; Chan, N.; et al. Advancing nutrition and obesity policy through cross-sector collaboration: The Local Farms-Healthy Kids initiative in Washington State. J. Hunger Environ. Nutr. 2013, 8, 171–186. [Google Scholar] [CrossRef]
- Breton, E.; De Leeuw, E. Theories of the policy process in health promotion research: A review. Health Promot. Int. 2011, 26, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Cairney, P. Standing on the shoulders of giants: How do we combine the insights of multiple theories in public policy studies? Policy Stud. J. 2013, 41, 1–21. [Google Scholar] [CrossRef]
- De Leeuw, E.; Clavier, C.; Breton, E. Health policy—Why research it and how: Health political science. Health Res. Policy Syst. 2014, 12, 55. [Google Scholar] [CrossRef] [PubMed]
- Knai, C.; Petticrew, M.; Mays, N.; Capewell, S.; Cassidy, R.; Cummins, S.; Eastmure, E.; Fafard, P.; Hawkins, B.; Jensen, J.; et al. Systems Thinking as a Framework for Analyzing Commercial Determinants of Health. Milbank Q. 2018, 96, 472–498. [Google Scholar] [CrossRef] [PubMed]
- Cairney, P. Understanding Public Policy: Theories and Issues; Palgrave MacMillan: Basingstoke, UK, 2012. [Google Scholar]
- John, P. Analysing Public Policy; Routledge: New York, NY, USA, 2012. [Google Scholar]
- Howlett, M.; Ramesh, M.; Perl, A. Studying Public Policy: Policy Cycles and Policy Subsystems; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Denzin, N.K.; Lincoln, Y.S. Introduction: The discipline and practice of qualitative research. In The Sage Handbook of Qualitative Research, 4th ed.; Denzin, N.K., Lincoln, D., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Breton, E.; Richard, L.; Gagnon, F.; Acques, M.J.; Bergeron, P. Fighting a tobacco-tax rollback: A political analysis of the 1994 cigarette contraband crisis in Canada. J. Public Health Policy 2006, 27, 77–99. [Google Scholar] [CrossRef] [PubMed]
- Breton, E.; Richard, L.; Gagnon, F.; Jacques, M.; Bergeron, P. Health promotion research and practice require sound policy analysis models: The case of Quebec’s Tobacco Act. Soc. Sci. Med. 2008, 67, 1679–1689. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, P.; Weible, C.M. Theories of the Policy Process; Westview Press: Oxford, UK, 2014. [Google Scholar]
- Jenkins-Smith, H.; Nohrstedt, D.; Weible, C.M.; Sabatier, P.A. The Advocacy Coalition Framework: Foundations, evolution and ongoing research. In Theories of the Policy Process, 3rd ed.; Sabatier, P.A., Weible, C.M., Eds.; Westview Press: Oxford, UK, 2014; pp. 183–224. [Google Scholar]
- Sabatier, P.A.; Weible, C.M. The Advocacy Coalition Framework: Innovations and clarifications. In Theories of the Policy Process, 2nd ed.; Sabatier, P., Ed.; Westview Press: Boulder, CO, USA, 2014. [Google Scholar]
- Weible, C.M.; Sabatier, P.A.; McQueen, K. Themes and variations: Taking stock of the Advocacy Coalition Framework. Policy Stud. J. 2009, 37, 121–140. [Google Scholar] [CrossRef]
- Gagnon, F.; Turgeon, J.; Dallaire, C. Healthy public policy: A conceptual cognitive framework. Health Policy 2007, 81, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Weible, C.M.; Sabatier, P. A guide to the Advocacy Coalition Framework. In Handbook of Public Policy Analysis: Theory, Politics and Methods; Fischer, F., Miller, G., Sidney, M., Eds.; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Schlager, E. A comparison of frameworks, theories and models of policy processes. In Theories of the Policy Process, 2nd ed.; Sabatier, P., Ed.; Westview Press: Boulder, CO, USA, 2007; pp. 293–320. [Google Scholar]
- Brunner, S. Understanding policy change: Multiple streams and emissions trading in Germany. Glob. Environ. Chang. 2008, 18, 501–507. [Google Scholar] [CrossRef]
- Ackrill, R.; Kay, A. Multiple streams in EU policy-making: The case of the 2005 sugar reform. J. Eur. Public Policy 2011, 18, 72–89. [Google Scholar] [CrossRef]
- Zohlnhöfer, R.; Herweg, N.; Huß, C. Bringing formal political institutions into the Multiple Streams Framework: An analytical proposal for comparative policy analysis. J. Comp. Policy Anal. 2016, 18, 243–256. [Google Scholar] [CrossRef]
- Ostrom, E. Institutional rational choice: An assessment of the Institutional Analysis and Development Framework. In Theories of the Policy Process; Sabatier, P., Ed.; Westview Press: Boulder, CO, USA, 2007. [Google Scholar]
- Ostrom, E.; Cox, M.; Schagler, E. An assessment fo the Institutional Analysis and Development Framework and introduction of the Socio-Ecological Systems Framework. In Theories of the Policy Process; Sabatier, P., Ed.; Westview Press: Boulder, CO, USA, 2014. [Google Scholar]
- Schlager, E. Policy making and collective action: Defining coalitions within the Advocacy Coalition Framework. Policy Sci. 1995, 28, 243–270. [Google Scholar] [CrossRef]
- Clement, F. Analysing decentralised natural resource governance: Proposition for a ‘politicised’ Institutional Analysis and Development Framework. Policy Sci. 2010, 43, 129–156. [Google Scholar] [CrossRef]
- Kingdon, J. Agendas, Alternatives and Public Policies, 2nd ed.; Little, Brown and Company: Boston, MA, USA, 1995. [Google Scholar]
- Zahariadis, N. The multiple streams, framework: Structure, limitations, prospects. In Theories of the Policy Process, 2nd ed.; Sabatier, P., Weible, C., Eds.; Westview Press: Boulder, CO, USA, 2007. [Google Scholar]
- Zahariadis, N. Ambiguity and multiple streams. In Theories of the Policy Process; Sabatier, P., Ed.; Westview Press: Boulder, CO, USA, 2014; pp. 25–58. [Google Scholar]
- Moynihan, D.P. Ambiguity in policy lessons: The agentification experience. Public Adm. 2006, 84, 1029–1050. [Google Scholar] [CrossRef]
- Mosier, S.L. Cookies, candy, and Coke: Examining state sugar-sweetened-beverage tax policy from a multiple streams approach. Int. Rev. Public Adm. 2013, 18, 93–120. [Google Scholar] [CrossRef]
- Ulmer, V.M.; Rathert, A.R.; Rose, D. Understanding policy enactment: The New Orleans fresh food retailer initiative. Am. J. Prev. Med. 2012, 43, S116–S122. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Andersen, D.F. Building confidence in causal maps generated from purposive text data: Mapping transcripts of the federal reserve. Syst. Dyn. Rev. 2012, 28, 311–328. [Google Scholar] [CrossRef]
- Ventana Systems. Vensim Personal Learning Edition. Available online: http://vensim.com/ (accessed on 16 May 2016).
- Allender, S.; Owen, B.; Kuhlberg, J.; Lowe, J.; Nagorcka-Smith, P.; Whelan, J.; Bell, C. A community based systems diagram of obesity causes. PLoS ONE 2015, 10, e0129683. [Google Scholar] [CrossRef] [PubMed]
- Paina, L.; Bennett, S.; Ssengooba, F.; Peters, D.H. Advancing the application of systems thinking in health: Exploring dual practice and its management in Kampala, Uganda. Health Res. Policy Syst. 2014, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- National Partnership Agreement on Preventive Health Implementation Working Group. National Partnership Agreement on Preventive Health National Implementation Plan 2009–2015; Department of Health: Canberra, Australia, 2009.
- Council of Australian Governments. National Partnership Agreement of Preventive Health: Implementation Overview. Available online: http://www.federalfinancialrelations.gov.au/content/npa/health_preventive/national_overview.pdf (accessed on 12 April 2015).
- Education and Training Committee. Victorian Parliamentary Inquiry into the Potential for Developing Opportunities for Schools to Become a Focus for Promoting Healthy Community Living; Parliament of Victoria: Melbourne, Australia, 2010.
- Department of Health. Joint Statement of Commitment Promoting Good Health at Work; Commonwealth Government of Australia: Canberra, Australia, 2012.
- WorkSafe. WorkHealth Check Research. Available online: http://www.worksafe.vic.gov.au/safety-and-prevention/health-and-wellbeing/research/charts (accessed on 17 March 2016).
- Department of Health and Human Services. Children’s Services Coordination Board. Available online: http://www.education.vic.gov.au/about/department/structure/Pages/coordboard.aspx (accessed on 23 May 2016).
- Cairney, P.; Fischer, M.; Ingold, K. Hydraulic fracturing policy in the United Kingdom: Coalition, cooperation, and opposition in the face of uncertainty. In Policy Debates on Hydraulic Fracturing: Comparing Coalition Politics in North America and Europe; Weible, C.M., Heikkila, T., Ingold, K., Fischer, M., Eds.; Palgrave Macmillan: New York, NY, USA, 2016. [Google Scholar]
- Maddison, S.; Denniss, R. An Introduction to Australian Public Policy: Theory and Practice; Cambridge University Press: Melbourne, Australia, 2013. [Google Scholar]
- Baker, P.; Hawkes, C.; Wingrove, K.; Demaio, A.R.; Parkhurst, J.; Thow, A.M.; Walls, H. What drives political commitment for nutrition? A review and framework synthesis to inform the United Nations Decade of Action on Nutrition. BMJ Glob. Health 2018, 3, e000485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahariadis, N. Delphic oracles: Ambiguity, institutions, and multiple streams. Policy Sci. 2016, 49, 3–12. [Google Scholar] [CrossRef]
- Meadows, D. Leverage Points: Places to Intervene in a System; Sustainability Institute: North Charleston, PA, USA, 1999. [Google Scholar]
- De Leeuw, E.; Breton, E. Policy change theories in health promotion research: A review. In Health Promotion and the Policy Process; Clavier, C., de Leeuw, E., Eds.; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Craig, R.L.; Felix, H.C.; Walker, J.F.; Phillips, M.M. Public health professionals as policy entrepreneurs: Arkansas’s childhood obesity policy experience. Am. J. Public Health 2010, 100, 2047–2052. [Google Scholar] [CrossRef] [PubMed]
- Dodson, E.A.; Fleming, C.; Boehmer, T.K.; Haire-Joshu, D.; Luke, D.A.; Brownson, R.C. Preventing childhood obesity through state policy: Qualitative assessment of enablers and barriers. J. Public Health Policy 2009, 30, S116–S176. [Google Scholar] [CrossRef] [PubMed]
- Gladwin, C.P.; Church, J.; Plotnikoff, R.C. Public policy processes and getting physical activity into Alberta’s urban schools. Can. J. Public Health 2008, 99, 332–338. [Google Scholar] [PubMed]
- Houlihan, B.; Green, M. The changing status of school sport and physical education: Explaining policy change. Sport Educ. Soc. 2006, 11, 73–92. [Google Scholar] [CrossRef]
- Khayesi, M.; Amekudzi, A.A. Kingdon’s multiple streams model and automobile dependence reversal path: The case of Curitiba, Brazil. J. Transp. Geogr. 2011, 19, 1547–1552. [Google Scholar] [CrossRef]
- Majone, G. Evidence, Argument, and Persuasion in the Policy Process; Yale University Press: New Haven, CT, USA, 1989. [Google Scholar]
- Schilling, J.; Keyes, S.D. The promise of Wisconsin’s 1999 comprehensive planning law: Land-use policy reforms to support active living. J. Health Politcs Policy Law 2008, 33, 455–496. [Google Scholar] [CrossRef] [PubMed]
- Phillpots, L. An analysis of the policy process for physical education and school sport: The rise and demise of school sport partnerships. Int. J. Sports Policy Politics 2012, 5, 193–211. [Google Scholar] [CrossRef]
- Payán, D.D.; Lewis, L.B.; Cousineau, M.R.; Nichol, M.B. Advocacy coalitions involved in California’s menu labeling policy debate: Exploring coalition structure, policy beliefs, resources, and strategies. Soc. Sci. Med. 2017, 177, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Gomez, E.J. Understanding the United States and Brazil’s response to obesity: Institutional conversion, policy reform, and the lessons learned. Glob. Health 2015, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Freudenberg, N.; Atkinson, S. Getting food policy on the Mayoral table: A comparison of two election cycles in New York and London. Public Health 2015, 129, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Milton, K.; Grix, J. Public health policy and walking in England-analysis of the 2008 ‘policy window’. BMC Public Health 2015, 15, 614. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Thornburn, M. Analysing policy change in Scottish physical education and school sport. J. Policy Res. Tour. Leis. Events 2011, 3, 298–315. [Google Scholar] [CrossRef]
- Cairney, P.; Geyer, R. Handbook on Complexity and Public Policy; Edward Elgar Publishing: Cheltenham, UK, 2015. [Google Scholar]
- Waqa, G.; Moodie, M.; Snowdon, W.; Latu, C.; Coriakula, J.; Allender, S.; Bell, C. Exploring the dynamics of food-related policymaking processes and evidence use in Fiji using systems thinking. Health Res. Policy Syst. 2017, 15, 74. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification strategies for establishing reliability and validity in qualitative research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods, 5th ed.; Sage Publications: London, UK, 2014. [Google Scholar]
- Yin, R.K. Case Study Research: Design and Methods; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Hawe, P. Lessons from complex interventions to improve health. Annu. Rev. Public Health 2015, 36, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Mialon, M.; Swinburn, B.; Allender, S.; Sacks, G. ‘Maximising shareholder value’: A detailed insight into the corporate political activity of the Australian food industry. Aust. N. Z. J. Public Health 2017, 41, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Nestle, M. Food Politics: How the Food Industry Influences Nutrition and Health; University of California Press: Oakland, CA, USA, 2007. [Google Scholar]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clarke, B.; Swinburn, B.; Sacks, G. Understanding Health Promotion Policy Processes: A Study of the Government Adoption of the Achievement Program in Victoria, Australia. Int. J. Environ. Res. Public Health 2018, 15, 2393. https://doi.org/10.3390/ijerph15112393
Clarke B, Swinburn B, Sacks G. Understanding Health Promotion Policy Processes: A Study of the Government Adoption of the Achievement Program in Victoria, Australia. International Journal of Environmental Research and Public Health. 2018; 15(11):2393. https://doi.org/10.3390/ijerph15112393
Chicago/Turabian StyleClarke, Brydie, Boyd Swinburn, and Gary Sacks. 2018. "Understanding Health Promotion Policy Processes: A Study of the Government Adoption of the Achievement Program in Victoria, Australia" International Journal of Environmental Research and Public Health 15, no. 11: 2393. https://doi.org/10.3390/ijerph15112393