From Surveillance to Intervention: Overview and Baseline Findings for the Active City of Liverpool Active Schools and SportsLinx (A-CLASS) Project

 , , and
, , and
Abstract
:1. Introduction
1.1. Generating an Evidence Base: Sportslinx
1.2. Designing Interventions
1.3. The Active City of Liverpool, Active Schools and SportsLinx (A-CLASS) Project
2. Materials and Methods
2.1. Study Design
2.2. Participants and Settings
2.2.1. Organisational Level
2.2.2. Individual Level
2.3. Intervention
2.3.1. Treatment Groups
2.3.2. Reward System
2.4. Measures
2.4.1. Anthropometry
2.4.2. Bone Mineral Content and Density
2.4.3. Body Composition
2.4.4. Fundamental Movement Skills
2.4.5. “Pre-Clinical” Cardiovascular Disease Risk Factors
2.4.6. Cardiorespiratory Fitness
2.4.7. Physical Activity
2.4.8. Physical Self-Perceptions and Self-Esteem
2.5. Sample Size and Statistical Power
2.6. Statistical Analysis
2.6.1. Baseline Descriptives and Cross-Sectional Analyses
2.6.2. Cluster Randomized Controlled Trial
3. Results
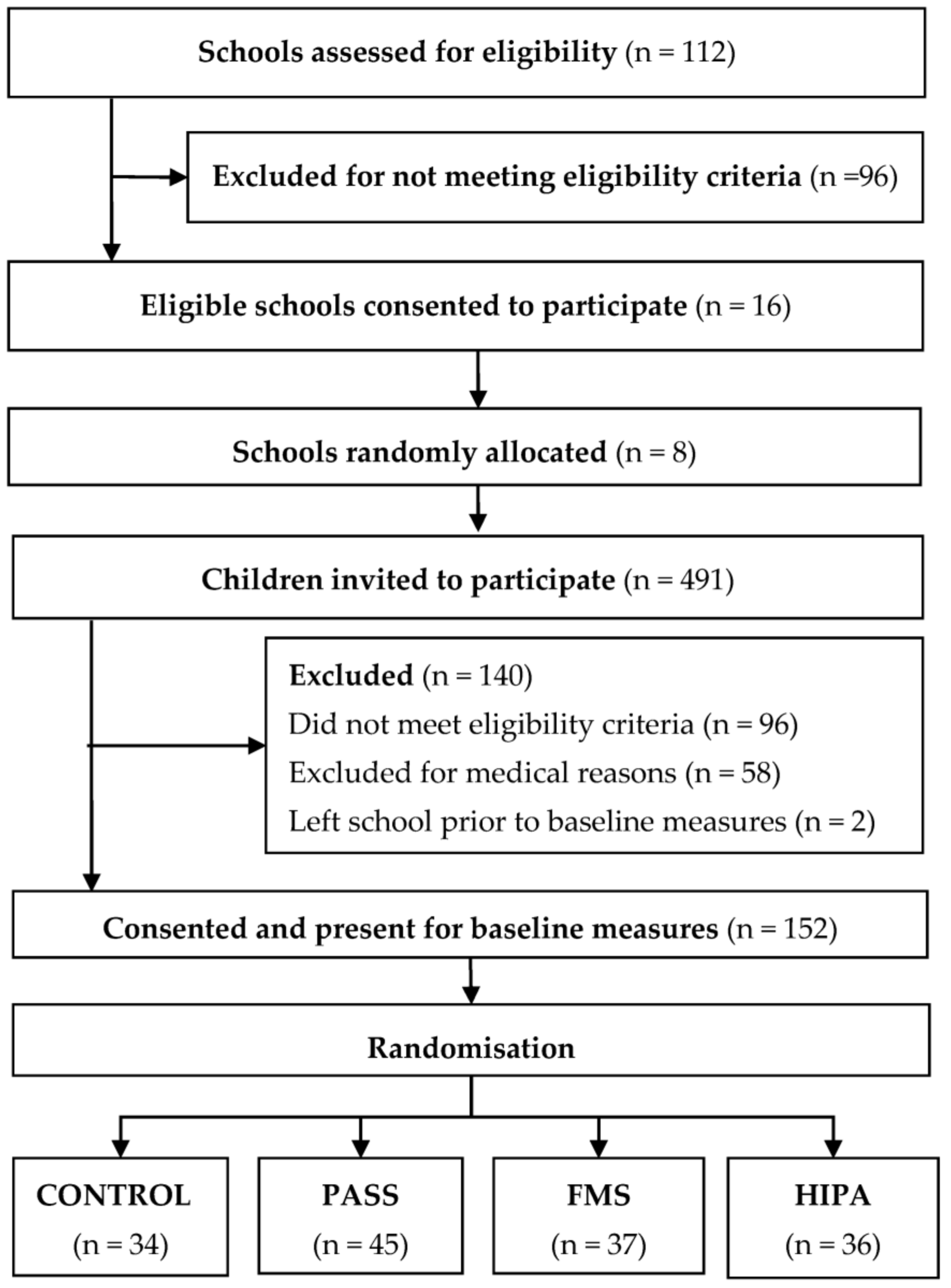
3.1. School and Participant Study Flow
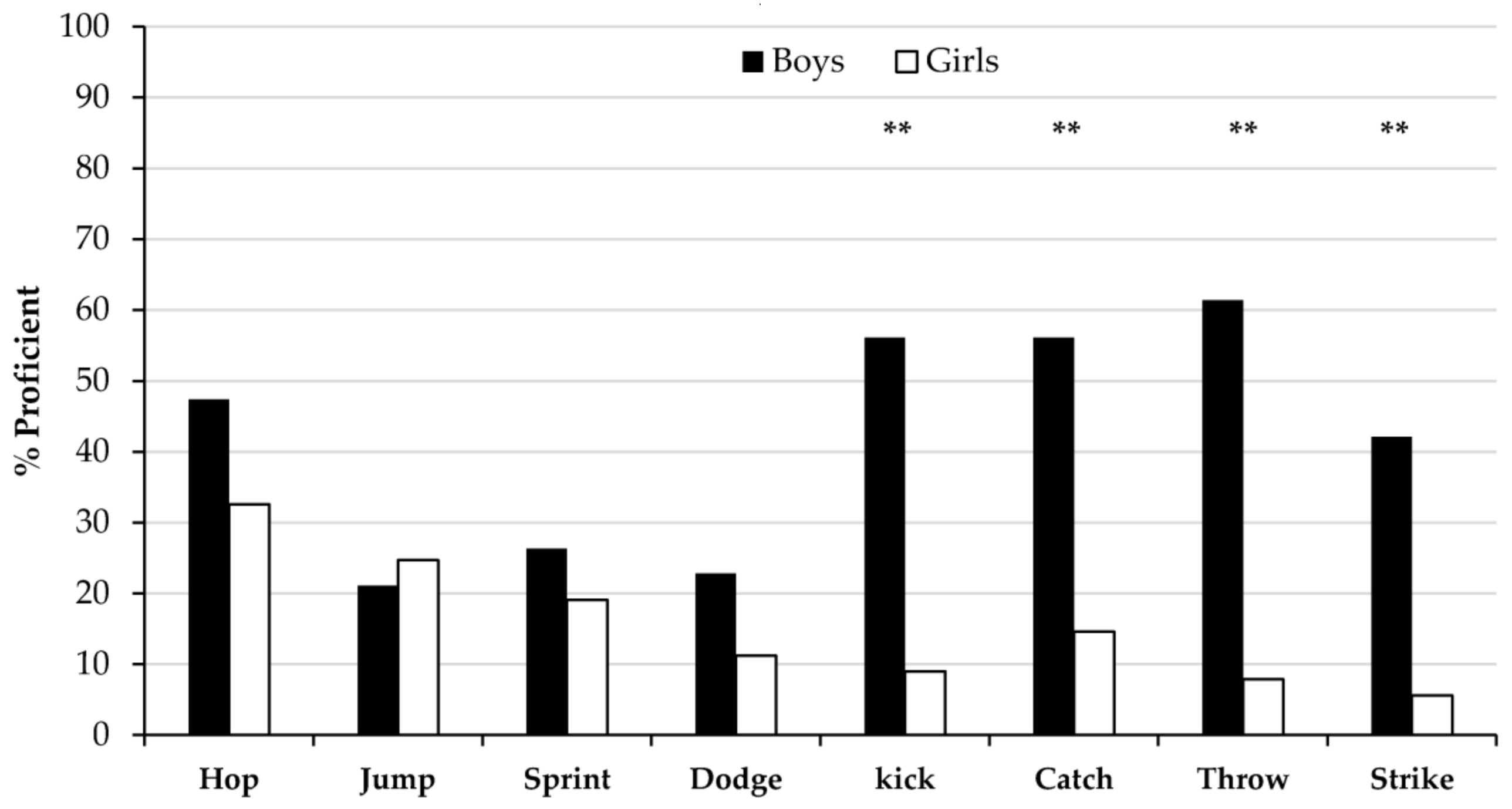
3.2. Baseline Characteristics
3.3. Main Analyses
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor-Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Sardinha, L.B.; Froberg, K.; Riddoch, C.J.; Page, A.S.; Anderssen, S.A. Fitness, fatness and clustering of cardiovascular risk factors in children from Denmark, Estonia and Portugal: The European Youth Heart Study. Int. J. Pediatr. Obes. 2008. [Google Scholar] [CrossRef] [PubMed]
- Riddoch, C.; Mahoney, C.; Murphy, N.; Boreham, C.; Cran, G. The Physical Activity Patterns of Northern Irish Schoolchildren Ages 11–16 Years. Pediatr. Exerc. Sci. 1991, 3, 300–309. [Google Scholar] [CrossRef]
- Taylor, S.R.; Stratton, G.; Hackett, A.F.; Lamb, L. Liverpool SportsLinx Project 01-3; Liverpool City Council: Liverpool, UK, 2003.
- Stratton, G.; Ridgers, N.D.; Fairclough, S.; Richardson, D.J. Physical Activity Levels of Normal-weight and Overweight Girls and Boys during Primary School Recess. Obesity 2007, 15, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Boddy, L.M.; Hackett, A.F.; Stratton, G. Associations between children’s socioeconomic status, weight status, and sex, with screen-based sedentary behaviours and sport participation. Int. J. Pediatr. Obes. 2009, 4, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Hackett, A.F.; Stratton, G. Changes in fitness, body mass index and obesity in 9–10 year olds. J. Hum. Nutr. Diet. 2010. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Boddy, L.M.; Hackett, A.F.; Stratton, G. Associations between children’s socioeconomic status, weight status, and sex, with screen-based sedentary behaviours and sport participation. Int. J. Pediatr. Obes. 2009. [Google Scholar] [CrossRef]
- Stratton, G. Promoting children’s physical activity in primary school: An intervention study using playground markings. Ergonomics 2000, 43, 1538–1546. [Google Scholar] [CrossRef] [PubMed]
- Stratton, G.; Mullan, E. The effect of multicolor playground markings on children’s physical activity level during recess. Prev. Med. 2005, 41, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Stratton, G.; Fairclough, S.J.; Twisk, J.W. Long-term effects of a playground markings and physical structures on children’s recess physical activity levels. Prev. Med. 2007, 44, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Stratton, G. Physical activity, fitness, and affective responses of normal-weight and overweight adolescents during physical education. Pediatr. Exerc. Sci. 2006, 18, 53–63. [Google Scholar] [CrossRef]
- Mears, R.; Jago, R. Effectiveness of after-school interventions at increasing moderate-to-vigorous physical activity levels in 5- to 18-year olds: A systematic review and meta-analysis. Br. J. Sports Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 28. [Google Scholar] [CrossRef] [PubMed]
- Kriemler, S.; Meyer, U.; Martin, E.; van Sluijs, E.M.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, B.; Wilkin, T. Lifestyle intervention in preschool children has little effect on obesity. BMJ 2012, 31, 344. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; McKenzie, T.L.; Beets, M.W.; Beighle, A.; Erwin, H.; Lee, S. Physical education’s role in public health. Steps forward and backward over 20 years and HOPE for the future. Res. Q. Exerc. Sport 2012, 83, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Department for Education and Skills and Department for Culture, Media and Sport. Learning through PE and Sport. A guide to the Physical Education, School Sport and Club Links Strategy. 2003. Available online: http://webarchive.nationalarchives.gov.uk/+/http:/www.culture.gov.uk/images/publications/learningthru.pdf (accessed on 9 October 2017).
- Department for Education and Skills and Department for Culture, Media and Sport. High Quality PE and Sport for Young People: A Guide to Recognising and Achieving High Quality PE and Sport in Schools and Clubs. 2004. Available online: http://www.gbwba.org.uk/gbwba/assets/File/8%20High%20Quality%20PE%20and%20Sport.pdf (accessed on 9 October 2017).
- Pate, R.R.; O’Neill, J.R. After-school interventions to increase physical activity among youth. Br. J. Sports Med. 2009, 43, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.; Stratton, G.; Foweather, L.; Henaghan, J.; McWhannell, N.; Stone, M.R. The Active City of Liverpool, Active Schools and SportsLinx (A-CLASS) Project. Educ. Health 2006, 24, 2. [Google Scholar]
- Medical Research Council (MRC). Developing and Evaluating Complex Interventions. 2006. Available online: https://www.mrc.ac.uk/documents/pdf/complex-interventions-guidance/ (accessed on 10 October 17).
- Foweather, L.; McWhannell, N.; Henaghan, J.; Lees, A.; Stratton, G.; Batterham, A. Effect of a 9-week after-school multiskills club on fundamental movement skill proficiency in 8 to 9 year old children: An exploratory trial. Percept. Mot. Skills 2008, 106, 745–754. [Google Scholar] [CrossRef] [PubMed]
- McWhannell, N.; Henaghan, J.L.; Foweather, L.; Doran, D.A.; Batterham, A.M.; Reilly, T.; Stratton, G. The effect of a 9-week physical activity programme on bone and body composition of children aged 10–11 years: An exploratory trial. Int. J. Sports Med. 2008, 29, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Henaghan, J.; McWhannell, N.; Foweather, L.; Cable, N.T.; Batterham, A.M.; Stratton, G.; George, K.P. The effect of structured exercise classes and a lifestyle intervention on cardiovascular risk factors in primary schoolchildren: An exploratory trial (The A-CLASS Project). Pediatr. Exerc. Sci. 2008, 20, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- Slotte, S.; Sääkslahti, A.; Metsämuuronen, J.; Rintala, P. Fundamental movement skill proficiency and body composition measured by dual energy X-ray absorptiometry in eight-year-old children. Early Child Dev. Care 2015. [Google Scholar] [CrossRef]
- Department for Communities and Local Government. English Indices of Deprivation 2010. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/6320/1870718.pdf (accessed on 18 February 2018).
- Chinn, S.; Rona, R.J. Letter to the Editor Re: International definitions of overweight and obesity for children: A lasting solution? Ann. Hum. Biol. 2004, 31, 695–696. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.; Ball, K.; Hume, C.; Booth, M.; Crawford, D. Outcomes of a group-randomized trial to prevent excess weight gain, reduce screen behaviours and promote physical activity in 10-year-old children: Switch-play. Int. J. Obes. 2008, 32, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Hepples, J.; Stratton, G. The Physical Activity Signposting Scheme (PASS): The A-CLASS Project. Educ. Health 2007, 25, 63–67. [Google Scholar]
- Hanford, C.; Haskins, D.; Hawkins, D.; Haydn-Davies, D.; Morley, D.; Stevenson, P. Mutli-Skill Resource Pack; Youth Sports Trust: Loughborough, 2005. [Google Scholar]
- Bandura, A. Social Foundations of thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Salmon, J.; Ball, K.; Crawford, D.; Booth, M.; Telford, A.; Hume, C.; Worsley, A. Reducing sedentary behaviour and increasing physical activity among 10-year-old children: Overview and process evaluation of the “Switch-Play” intervention. Health Promot. Int. 2005. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.; Burns, C.F.; McGuinness, M.; Heslin, J.; Murphy, N.M. Influence of a health education intervention on physical activity and screen time in primary school children: ‘Switch Off–Get Active’. J. Sci. Med. Sport 2006, 9, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Department for Education (DFE). The National Curriculum. Available online: https://www.gov.uk/national-curriculum (accessed on 9 October 2017).
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sport Exerc. 2002, 34, 689–694. [Google Scholar]
- Lewieki, E.M. Update on bone density testing. Curr. Osteoporos. Rep. 2005, 3, 136–142. [Google Scholar] [CrossRef]
- Sopher, A.B.; Thornton, J.C.; Wang, J.; Pierson, R.N.; Heymsfield, S.B.; Horlick, M. Measurement of percentage of body fat in 411 children and adolescents: A comparison of dual-energy X-ray absorptiometry with a four-compartment model. Pediatrics 2004, 113, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. International Standards for Anthropometric Assessment; ISAK: Potchefstroom, South Africa, 2006. [Google Scholar]
- Hands, B.; Larkin, D. Gender bias in measurement of movement. ACHPER 1997, 44, 12–16. [Google Scholar]
- Knudson, D.V. Qualitative Diagnosis of Human Movement: Improving Performance in Sport and Exercise; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Nsw Department of Education and Training. Get Skilled: Get Active. A K-6 Resource to Support the Teaching of Fundamental Movement Skills; Department of Education and Training: Ryde, Australia, 2000; ISBN 0731358848.
- Victoria Department of Education. Fundamental Motor Skills: A Manual for Classroom Teachers; Department of Education, Victoria: Melbourne, Australia, 1996; ISBN 9780730689164.
- Booth, M.L.; Macaskill, P.; Phongsavan, P.; McLellan, L.; Okely, T. Methods of the NSW Schools Fitness and Physical Activity Survey, 1997. J. Sci. Med. Sport 1998. [Google Scholar] [CrossRef]
- Van Beurden, E.; Barnett, L.M.; Zask, A.; Dietrich, U.C.; Brooks, L.O.; Beard, J. Can we skill and activate children through primary school physical education lessons? “Move it Groove it”—A collaborative health promotion intervention. Prev Med. 2003, 36, 493–501. Available online: http://www.sciencedirect.com/science/article/pii/S0091743502000440?via%3Dihub (accessed on 9 October 2017). [CrossRef]
- Payne, V.G.; Isaacs, L.D. Human Motor Development: A Lifespan Approach, 9th ed.; McGraw-Hill: New York, NY, USA, 2017; ISBN 9780078022494. [Google Scholar]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Schiller, N.B.; Shah, P.M.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of two-dimensional echocardiograms. J. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison of necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- De Simone, G.; Kizer, J.R.; Chinali, M.; Roman, M.J.; Bella, J.N.; Best, L.G.; Lee, E.T.; Devereux, R.B. Normalization for body size and population-attributable risk of left ventricular hypertrophy: The Strong Heart Study. Am. J. Hypertens. 2005, 18, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, N.; Welsman, J.R. Aerobic fitness. In Paediatric Exercise Science and Medicine; Armstrong, N., van Mechelen, W., Eds.; Oxford University Press: Oxford, UK, 2000; pp. 137–179. ISBN 9780199232482. [Google Scholar]
- Jones, A.M.; Doust, J.H. A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J. Sports Sci. 1996, 14, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Sjostrom, M.; Yngve, A.; Poortvliet, E.; Nilsson, A.; Froberg, K.; Wedderkopp, N.; Westerterp, K. Physical activity assessed by activity monitor and doubly labeled water in children. Med. Sci. Sports Exerc. 2001, 33, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Puyau, M.R.; Adolph, A.L.; Vohra, F.A.; Butte, N.F. Validation and calibration of physical activity monitors in children. Obes. Res. 2002, 10, 150–157. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Bakker, I.; Hopman-Rock, M.; Hirasing, R.A.; van Mechelen, W. Clinimetric review of motion sensors in children and adolescents. J. Clin. Epidemiol. 2006, 59, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Plasqui, G.; Westerterp, K.R. Physical activity assessment with accelerometers: An evaluation against doubly labeled water. Obesity (Silver Spring) 2007, 15, 2371–2379. [Google Scholar] [CrossRef] [PubMed]
- Baquet, G.; Stratton, G.; Van Praagh, E.; Berthoin, S. Improving physical activity assessment in prepubertal children with high-frequency accelerometry monitoring: A methodological issue. Prev. Med. 2007, 44, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Mattocks, C.; Ness, A.; Leary, S.; Tilling, K.; Blair, S.N.; Shield, J.; Deere, K.; Saunders, J.; Kirkby, J.; Davey Smith, G.; et al. Use of accelerometers in a large field-based study of children: Protocols, design issues, and effects on precision. J. Phys. Act. Health 2008, 5 (Suppl. 1), S98–S111. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of accelerometer cut points for predicting activity intensity in youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, J. A study of children’s physical self-perceptions using an adapted Physical Self-Perception Profile questionnaire. Pediatr. Exerc. Sci. 1995, 7, 132–151. [Google Scholar] [CrossRef]
- Welk, G.; Eklund, B. Validation of the Children and Youth Physical Self Perceptions Profile for young children. Psychol. Sport Exerc. 2005, 6, 51–65. [Google Scholar] [CrossRef]
- Southall, J.; Okely, A.D.; Steele, J. Actual and perceived physical competence in overweight and nonoverweight children. Pediatr. Exerc. Sci. 2004, 16, 15–24. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Till, K.; Ogilvie, P.; Turner, G. Influences of gender and socioeconomic status on the motor proficiency of children in the UK. Hum. Mov. Sci. 2015, 44, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental movement skills and weight status in British primary school children. Eur. J. Sport Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Hume, C.; Okely, A.; Bagley, S.; Telford, A.; Booth, M.; Crawford, D.; Salmon, J. Does weight status influence associations between children’s fundamental movement skills and physical activity? Res. Q. Exerc. Sport 2008, 79, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Barnett, L.; Espinel, P.; Okely, A.D. Thirteen-year trends in child and adolescent fundamental movement skills: 1997–2010. Med. Sci. Sports Exerc. 2013, 45, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J.D. Understanding Motor Development: Infants, Children, Adolescents, Adults, 7th ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Holfelder, B.; Schott, N. Relationship of fundamental movement skills and physical activity in children and adolescents: A systematic review. Psychol. Sport Exerc. 2014, 15, 382–391. [Google Scholar] [CrossRef]
- Logan, S.W.; Kipling Webster, E.; Getchell, N.; Pfeiffer, K.A.; Robinson, L.E. Relationship between fundamental motor skill competence and physical activity during childhood and adolescence: A systematic review. Kinesiol. Rev. 2015, 4, 416–426. [Google Scholar] [CrossRef]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Lai, S.K.; Veldman, S.L.; Hardy, L.L.; Cliff, D.P.; Morgan, P.J.; Zask, A.; Lubans, D.R.; Shultz, S.P.; Ridgers, N.D.; et al. Correlates of gross motor competence in children and adolescents: A systematic review and meta-analysis. Sports Med. 2016, 46, 1663–1688. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Cale, L.; Musson, H. The predicament of primary physical education: A consequence of ‘insufficient’ ITT and ‘ineffective’ CPD. Phys. Educ. Sport Pedag. 2012, 17, 367–381. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.; Bourke, S. Non-specialist teachers’ confidence to teach PE: The nature and influence of personal school experiences in PE. Phys. Educ. Sport Pedag. 2008, 13, 1–29. [Google Scholar] [CrossRef]
- Lander, N.J.; Barnett, L.M.; Brown, H.; Telford, A. Physical education teacher training in fundamental movement skills makes a difference to instruction and assessment practices. J. Teach. Phys. Ed. 2015, 34, 548–556. [Google Scholar] [CrossRef]
- Lander, N.; Eather, N.; Morgan, P.J.; Salmon, J.; Barnett, L.M. Characteristics of teacher training in school-based physical education interventions to improve fundamental movement skills and/or physical activity: A systematic review. Sports Med. 2017, 47, 135–161. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.J.; Fairclough, S.J.; Ridgers, N.D.; Porteous, C. An observational assessment of physical activity levels and social behaviour during elementary school recess. Health Educ. J. 2013, 72, 254–262. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Fairclough, S.J.; Stratton, G. Variables associated with children’s physical activity levels during recess: The A-CLASS project. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Zabinski, M.F.; Saelens, B.E.; Stein, R.I.; Hayden-Wade, H.A.; Wilfley, D.E. Overweight children’s barriers to and support for physical activity. Obesity 2003, 11, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Hayden-Wade, H.A.; Stein, R.I.; Ghaderi, A.; Saelens, B.E.; Zabinski, M.F.; Wilfley, D.E. Prevalence, characteristics, and correlates of teasing experiences among overweight children vs. non-overweight peers. Obesity 2005, 13, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Bryant, E.; Stodden, D. Low fundamental movement skill proficiency is associated with high BMI and body fatness in girls but not boys aged 6–11 years old. J. Sports Sci. 2017, 35, 2135–2141. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.L.; Chey, T. Relationships between body composition and fundamental movement skills among children and adolescents. Res. Q. Exerc. Sport 2004, 75, 238–247. [Google Scholar] [CrossRef] [PubMed]
- D’Hondt, E.; Deforche, B.; De Bourdeaudhuij, I.; Lenoir, M. Relationship between motor skill and body mass index in 5-to 10-year-old children. Adapt. Phys. Act. Q. 2009, 26, 21–37. [Google Scholar] [CrossRef]
- McGraw, B.; McClenaghan, B.A.; Williams, H.G.; Dickerson, J.; Ward, D.S. Gait and postural stability in obese and nonobese prepubertal boys. Arch. Phys. Med. Rehabil. 2000, 81, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Stovitz, S.D.; Pardee, P.E.; Vazquez, G.; Duval, S.; Schwimmer, J.B. Musculoskeletal pain in obese children and adolescents. Acta Paediatr. 2008, 97, 489–931. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Skill | Task | Criteria |
|---|---|---|
| Hop | Hop as fast as you can over a distance of 15 m | 1. Support leg is bent in preparation and then straightens to push off 2. Takes off and lands on forefoot 3. Swing leg moves in rhythm with support leg 4. Able to hop on both right and left legs 5. Head and trunk stable with eyes focused forward 6. Arms bent and move to assist leg action |
| Vertical Jump | Jump and touch the wall as high as you can | 1. Eyes focused forwards or upwards throughout the jump 2. Crouch with knees bent and arms behind the body 3. Forceful upward thrust of arms as legs straighten to take off 4. Legs straighten in the air 5. Contact ground with front part of feet and bend knees to absorb force of landing 6. Balanced landing with no more than one step in any direction |
| Dodge | Dodge through a series of cones placed in zig-zag formation, 3 m apart | 1. Bend knees during change of direction 2. Push off on outside of foot when changing direction 3. Body lowered during change of direction 4. Eyes focused in direction of travel 5. Can dodge to either side 6. Arms move to assist action |
| Sprint run | Run a distance of 30 m as fast as possible | 1. Lands on balls of feet 2. Eyes focused forward, head and trunk stable throughout the run 3. High knee lift (thigh almost parallel to the ground) 4. Knees bend at right angles during the recovery phase 5. Arms bent at least 90 degrees 6. Arms driving forward and back in opposition to legs |
| Kick | Kick a size 4 football towards a target as hard as possible | 1. Eyes are focussed on the ball throughout the kick 2. Forward and sideward swing of arm opposite kicking leg 3. Step forward with non-kicking foot placed near the ball 4. Hip extension and knee flexion of at least 90 degrees during preliminary kicking movement 5. Contact the ball with the top of the foot (a “shoelace” or instep kick) 6. Kicking leg follows through high towards the target after ball contact |
| Catch | Catch a tennis ball thrown underarm between 2–3 m high, and from a distance of 10 m | 1. Eyes are focused on the ball throughout the catch 2. Feet move to put body in line with object 3. Hands move to meet ball 4. Hands and fingers positioned correctly to catch the ball 5. Catch and control the ball with hands only (well-timed closure) 6. Elbows bend to absorb force of the ball |
| Overarm Throw | Throw a tennis ball overarm as far as possible | 1. Eyes are focused on the target throughout the throw 2. Stand side-on to the target 3. Arm moves in a down-ward and backward arc 4. Step towards the target with foot opposite throwing arm during the throw 5. Hip then shoulders rotate forward 6. Throwing arm follows through down and across the body |
| Strike | Using a t-ball stand and a foam baseball bat, hit a tennis ball as far as possible | 1. Stand side-on to target 2. GRIP: hands next to each other, hand closest to handle end matches front foot 3. Front foot steps forward (weight transfers from back to front) 4. Hips then shoulders rotate forwards 5. Ball contact made on front foot with straight arms 6. Follow through with bat around body |
| Characteristics | Total (n = 146) | Boys (n = 57) | Girls (n = 89) | p-Value |
|---|---|---|---|---|
| Anthropometry | ||||
| Age (years) | 9.6 (0.3) | 9.6 (0.3) | 9.6 (0.3) | 0.913 |
| Maturity offset (years) | −2.4 (0.8) | −3.3 (0.5) | −1.9 (0.5) | 0.000 ** |
| Stature (cm) | 138.5 (6.4) | 138.9 (6.5) | 138.3 (6.3) | 0.556 |
| Mass (kg) | 36.7 (8.4) | 37.0 (8.9) | 36.5 (8.1) | 0.737 |
| BMI (kg/m2) | 18.9 (3.2) | 18.9 (3.4) | 18.9 (3.1) | 0.997 |
| Body fat (%) | 27.6 (6.5) | 24.9 (6.9) | 29.3 (5.7) | 0.000 ** |
| Fundamental movement skills | ||||
| Hop | 4.0 (1.2) | 4.2 (1.2) | 3.9 (1.2) | 0.126 |
| Vertical jump | 4.0 (0.8) | 4.1 (0.8) | 4.0 (0.8) | 0.666 |
| Sprint run | 3.5 (1.1) | 3.5 (1.2) | 3.5 (1.0) | 0.934 |
| Dodge | 2.8 (1.4) | 3.3 (1.4) | 2.5 (1.4) | 0.001 ** |
| Kick | 3.5 (1.5) | 4.5 (1.4) | 2.9 (1.1) | 0.000 ** |
| Catch | 3.4 (1.7) | 4.5 (1.3) | 2.7 (1.6) | 0.000 ** |
| Throw | 3.3 (1.7) | 4.7 (1.2) | 2.4 (1.3) | 0.000 ** |
| Strike | 3.4 (1.5) | 4.4 (1.2) | 2.9 (1.2) | 0.000 ** |
| Locomotor skills | 14.4 (3.3) | 15.1 (3.4) | 13.9 (3.1) | 0.028 * |
| Object control skills | 13.6 (5.1) | 18.2 (3.7) | 10.7 (3.4) | 0.000 ** |
| Total skill score | 28.0 (7.1) | 33.3 (5.9) | 24.6 (5.5) | 0.000 ** |
| Predictor | β | SE | 95% CI | p | r2 | sri2 |
|---|---|---|---|---|---|---|
| Total skill score | −0.27 | 0.08 | −0.43 to −0.12 | 0.001 | 40.7% | 5.2% |
| Locomotor skills | −0.88 | 0.14 | −1.14 to −0.61 | 0.000 | 50.6% | 15.0% |
| Object-control skills | 0.26 | 0.12 | 0.02 to 0.51 | 0.036 | 2% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McWhannell, N.; Foweather, L.; Graves, L.E.F.; Henaghan, J.L.; Ridgers, N.D.; Stratton, G. From Surveillance to Intervention: Overview and Baseline Findings for the Active City of Liverpool Active Schools and SportsLinx (A-CLASS) Project. Int. J. Environ. Res. Public Health 2018, 15, 582. https://doi.org/10.3390/ijerph15040582
McWhannell N, Foweather L, Graves LEF, Henaghan JL, Ridgers ND, Stratton G. From Surveillance to Intervention: Overview and Baseline Findings for the Active City of Liverpool Active Schools and SportsLinx (A-CLASS) Project. International Journal of Environmental Research and Public Health. 2018; 15(4):582. https://doi.org/10.3390/ijerph15040582
Chicago/Turabian StyleMcWhannell, Nicola, Lawrence Foweather, Lee E. F. Graves, Jayne L. Henaghan, Nicola D. Ridgers, and Gareth Stratton. 2018. "From Surveillance to Intervention: Overview and Baseline Findings for the Active City of Liverpool Active Schools and SportsLinx (A-CLASS) Project" International Journal of Environmental Research and Public Health 15, no. 4: 582. https://doi.org/10.3390/ijerph15040582