
Ambient Temperature and Stroke Occurrence: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
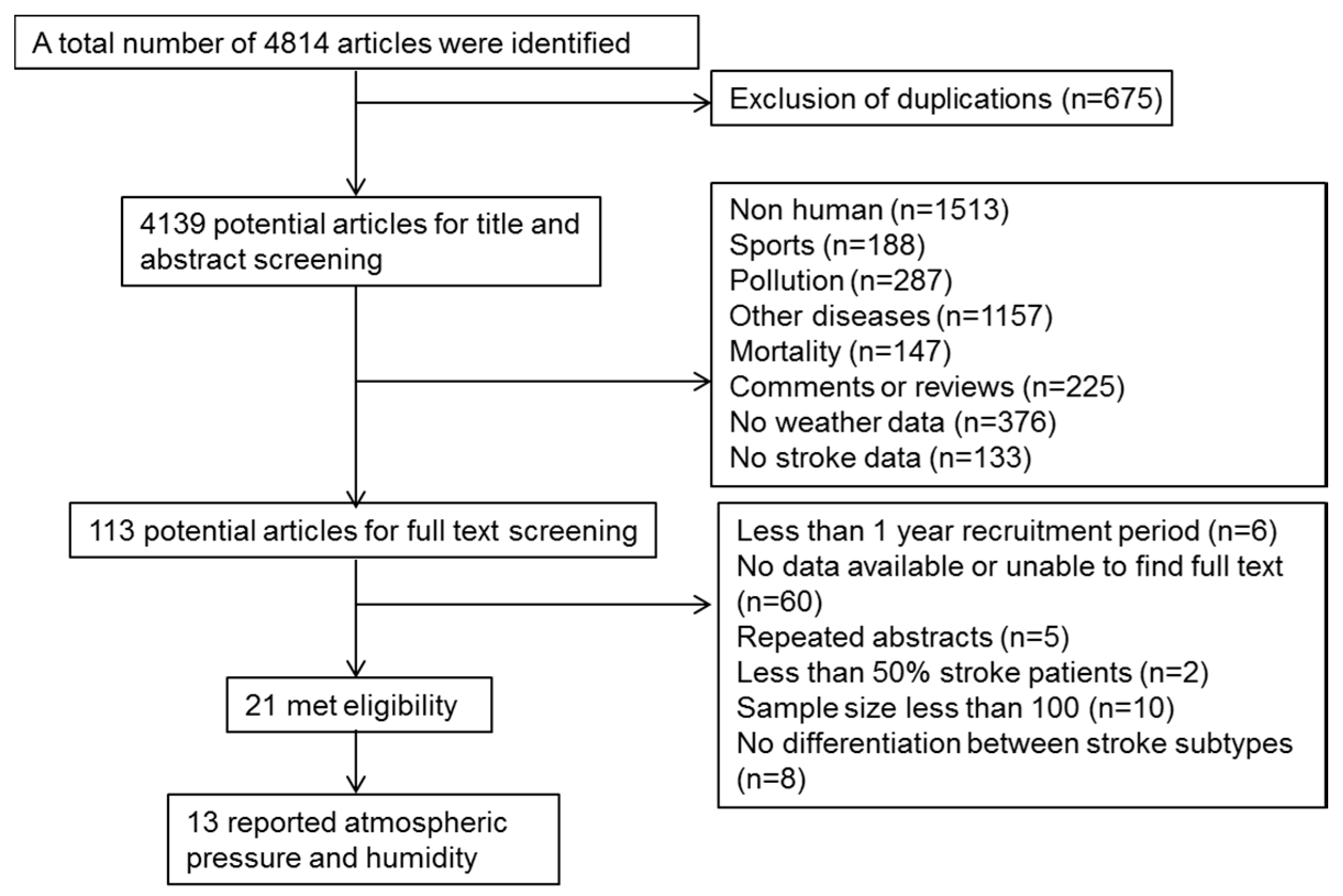
2. Materials and Methods
2.1. Study Eligibility Criteria
2.2. Databases and Sources
2.3. Data Collection and Extraction
2.4. Data Analysis
3. Results
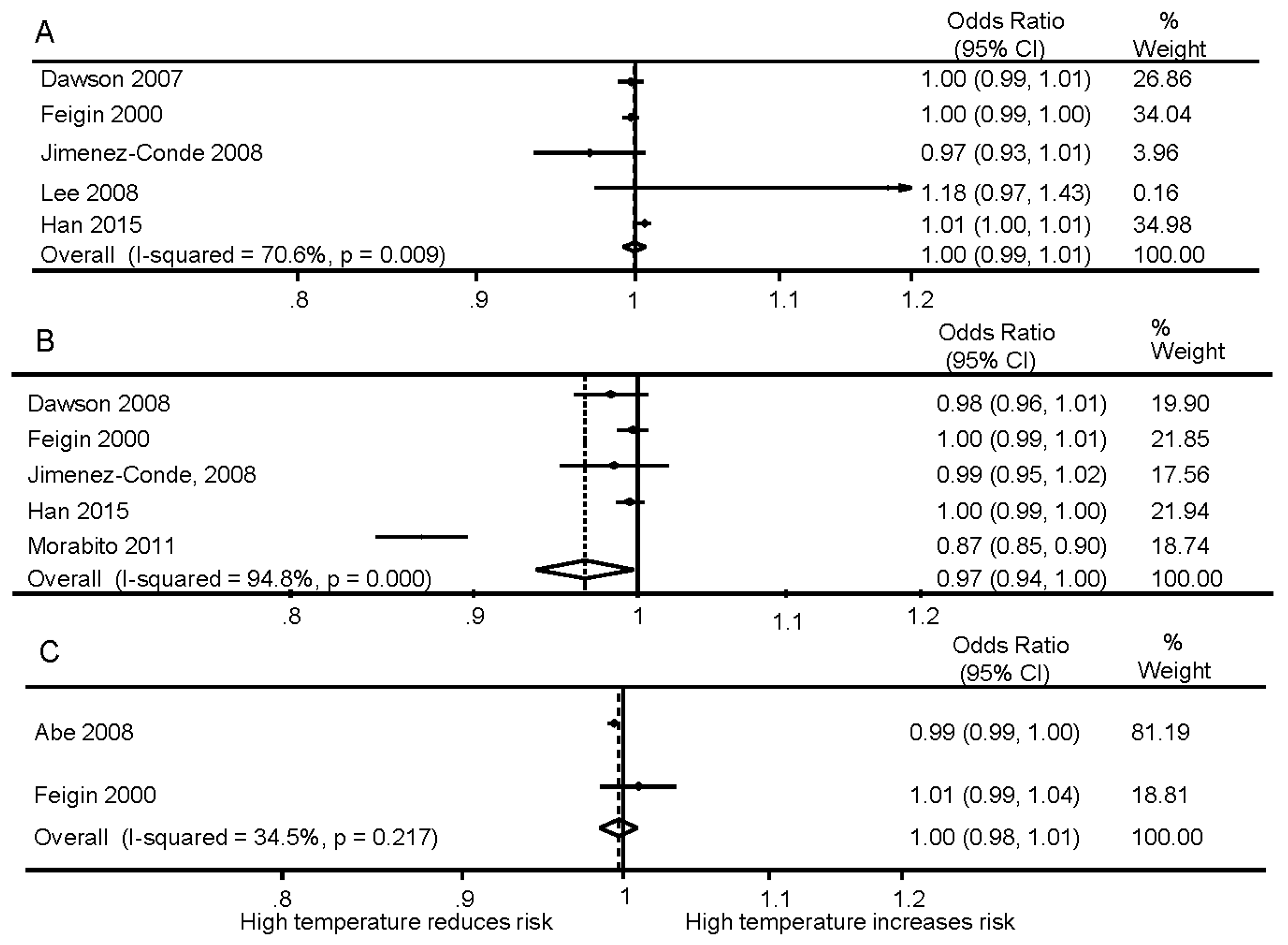
3.1. Ischemic Stroke
3.1.1. Mean, Minimum and Maximum Temperature
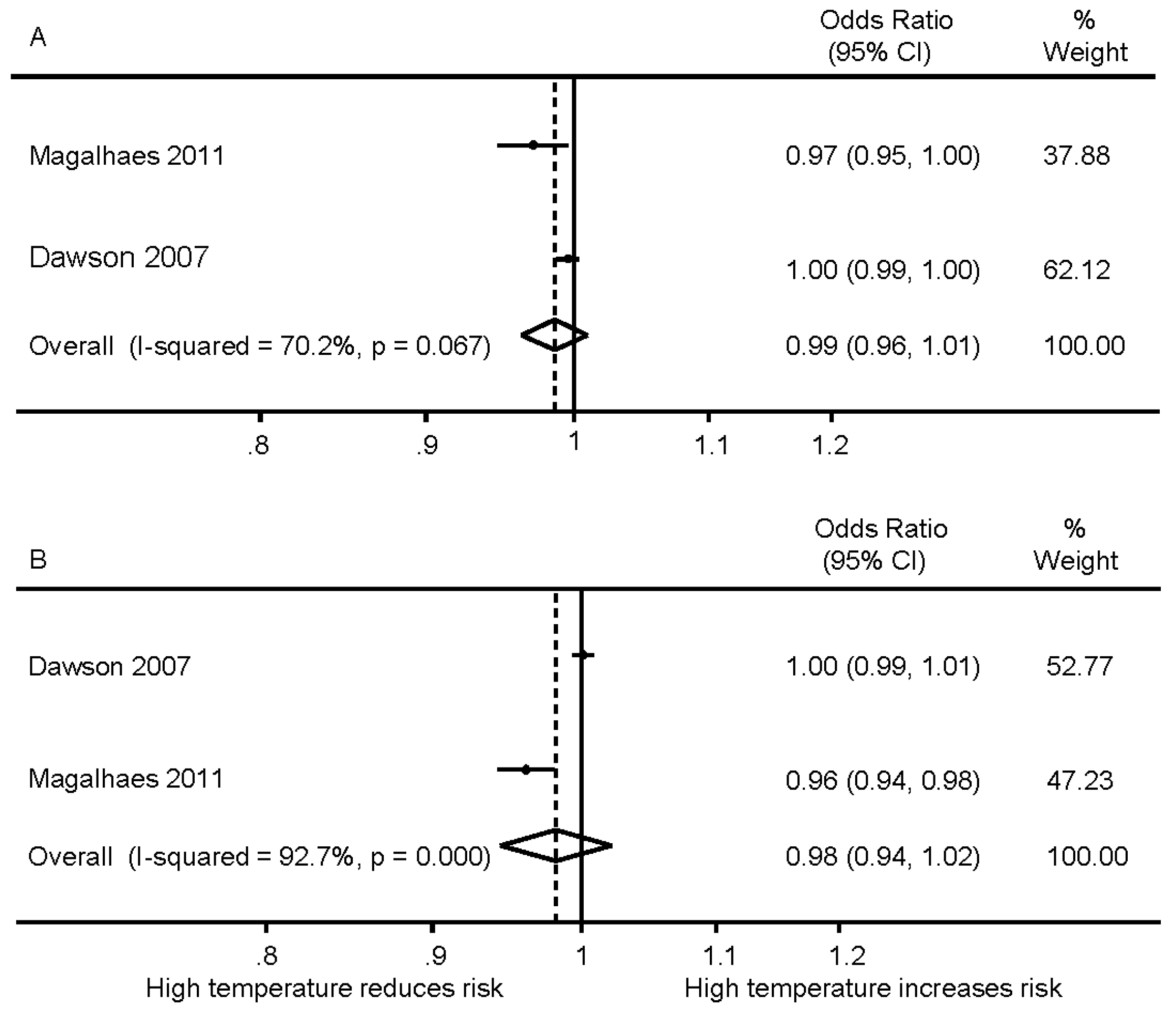
3.1.2. Subgroup by Sex and Age
3.1.3. Temperature Change
3.2. Intracerebral Hemorrhage
3.2.1. Mean, Minimum and Maximum Temperature
3.2.2. Subgroup by Sex and Age
3.2.3. Temperature Change
3.3. Subarachnoid Hemorrhage
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Murray, C.J.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Keatinge, W.R.; Coleshaw, S.R.; Cotter, F.; Mattock, M.; Murphy, M.; Chelliah, R. Increases in platelet and red cell counts, blood viscosity, and arterial pressure during mild surface cooling: Factors in mortality from coronary and cerebral thrombosis in winter. Br. Med. J. 1984, 289, 1405–1408. [Google Scholar] [CrossRef]
- Woodhouse, P.R.; Khaw, K.-T.; Plummer, M. Seasonal variation of blood pressure and its relationship to ambient temperature in an elderly population. J. Hypertens. 1993, 11, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Orlandini, S.; Maracchi, G.; Gensini, G.F.; Modesti, P.A. A synoptic approach to weather conditions discloses a relationship with ambulatory blood pressure in hypertensives. Am. J. Hypertens. 2008, 21, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Hubert, G.J.; Müller-Barna, P.; Haberl, R.L. Unsolved issues in the management of high blood pressure in acute ischemic stroke. Int. J. Hypertens. 2013, 2013, 349782. [Google Scholar] [CrossRef] [PubMed]
- Bath, P.; Chalmers, J.; Powers, W.; Beilin, L.; Davis, S.; Lenfant, C.; Mancia, G.; Neal, B.; Whitworth, J.; Zanchetti, A.; et al. International Society of Hypertension (ISH): Statement on the management of blood pressure in acute stroke. J. Hypertens. 2003, 21, 665–672. [Google Scholar] [PubMed]
- Qureshi, A.I.; Ezzeddine, M.A.; Nasar, A.; Suri, M.F.; Kirmani, J.F.; Hussein, H.M.; Divani, A.A.; Reddi, A.S. Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Am. J. Emerg. Med. 2007, 25, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Korja, M.; Silventoinen, K.; Laatikainen, T.; Jousilahti, P.; Salomaa, V.; Hernesniemi, J.; Kaprio, J. Risk factors and their combined effects on the incidence rate of subarachnoid hemorrhage—A population-based cohort study. PLoS ONE 2013, 8, e73760. [Google Scholar] [CrossRef] [PubMed]
- Kyobutungi, C.; Grau, A.; Stieglbauer, G.; Becher, H. Absolute temperature, temperature changes and stroke risk: A case-crossover study. Eur. J. Epidemiol. 2005, 20, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Cevik, Y.; Dogan, N.O.; Das, M.; Ahmedali, A.; Kul, S.; Bayram, H. The association between weather conditions and Stroke admissions in Turkey. Int. J. Biometeorol. 2015, 59, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Ohshige, K.; Hori, Y.; Tochikubo, O.; Sugiyama, M. Influence of weather on emergency transport events coded as Stroke: Population-based study in Japan. Int. J. Biometeorol. 2006, 50, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Ohwaki, K.; Yano, E.; Murakami, H.; Nagashima, H.; Nakagomi, T. Meteorological factors and the onset of hypertensive intracerebral hemorrhage. Int. J. Biometeorol. 2004, 49, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Barnett, A.G.; Hu, W.; Tong, S. Temperature variation and emergency hospital admissions for Stroke in Brisbane, Australia, 1996–2005. Int. J. Miometeorol. 2009, 53, 535–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.Y.; Chang, S.F.; Su, C.L. Weather and Stroke in a subtropical area: Ilan, Taiwan. Stroke 1995, 26, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Conde, J.; Ois, A.; Gomis, M.; Rodriguez-Campello, A.; Cuadrado-Godia, E.; Subirana, I.; Roquer, J. Weather as a trigger of Stroke. Daily meteorological factors and incidence of stroke subtypes. Cerebrovasc. Dis. 2008, 26, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Jeong, T.S.; Park, C.W.; Yoo, C.J.; Kim, E.Y.; Kim, Y.B.; Kim, W.K. Association between the daily temperature range and occurrence of spontaneous intracerebral hemorrhage. J. Cerebrovasc. Endovasc. Neurosurg. 2013, 15, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.W.; Ma, M.C.; Lin, H.J.; Chen, C.H. Ambient temperature and spontaneous intracerebral haemorrhage: A cross-sectional analysis in Tainan, Taiwan. BMJ Open 2012, 2, e000842. [Google Scholar] [CrossRef] [PubMed]
- Cowperthwaite, M.C.; Burnett, M.G. An analysis of admissions from 155 United States hospitals to determine the influence of weather on stroke incidence. J. Neurosci. 2011, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Wroe, S.J.; Slattery, J.; Warlow, C.P. Is stroke incidence related to season or temperature? The oxfordshire community stroke project. Lancet 1996, 347, 934–936. [Google Scholar] [CrossRef]
- Field, T.S.; Hill, M.D. Weather, chinook, and stroke occurrence. Stroke 2002, 33, 1751–1757. [Google Scholar] [CrossRef] [PubMed]
- Goggins, W.B.; Woo, J.; Ho, S.; Chan, E.Y.; Chau, P.H. Weather, season, and daily stroke admissions in Hong Kong. Int. J. Biometeorol. 2012, 56, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Lian, H.; Ruan, Y.; Liang, R.; Liu, X.; Fan, Z. Short-term effect of ambient temperature and the risk of stroke: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2015, 12, 9068–9088. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Nikitin, Y.P.; Bots, M.L.; Vinogradova, T.E.; Grobbee, D.E. A population-based study of the associations of stroke occurrence with weather parameters in Siberia, Russia (1982–1992). Eur. J. Neurol. 2000, 7, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- De Steenhuijsen Piters, W.A.; Algra, A.; van den Broek, M.F.; Dorhout Mees, S.M.; Rinkel, G.J. Seasonal and meteorological determinants of aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. J. Neurol. 2013, 260, 614–619. [Google Scholar] [CrossRef] [PubMed]
- McArthur, K.; Dawson, J.; Walters, M. What is it with the weather and stroke? Expert Rev. Neurother. 2010, 10, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Ohde, S.; Ishimatsu, S.; Ogata, H.; Hasegawa, T.; Nakamura, T.; Tokuda, Y. Effects of meteorological factors on the onset of subarachnoid hemorrhage: A time-series analysis. J. Clin. Neurosci. 2008, 15, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Weir, C.; Wright, F.; Bryden, C.; Aslanyan, S.; Lees, K.; Bird, W.; Walters, M. Associations between meteorological variables and acute stroke hospital admissions in the west of Scotland. Acta Neurol. Scand. 2008, 117, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Hu, C.J.; Chen, C.S.; Lin, H.C. Seasonal variation in ischemic stroke incidence and association with climate: A six-year population-based study. Chronobiol. Int. 2008, 25, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Magalhaes, R.; Silva, M.C.; Correia, M.; Bailey, T. Are stroke occurrence and outcome related to weather parameters? Results from a population-based study in northern Portugal. Cerebrovasc. Dis. 2011, 32, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Vallorani, R.; Modesti, P.A.; Gensini, G.F.; Orlandini, S. Innovative approaches helpful to enhance knowledge on weather-related stroke events over a wide geographical area and a large population. Stroke 2011, 42, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Han, M.H.; Yi, H.J.; Kim, Y.S.; Kim, Y.S. Effect of seasonal and monthly variation in weather and air pollution factors on stroke incidence in Seoul, Korea. Stroke 2015, 46, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.; Damasceno, A.; Carrilho, C.; Lobo, V.; Lopes, H.; Madede, T.; Pravinrai, P.; Silva-Matos, C.; Diogo, D.; Azevedo, A.; et al. Triggering of stroke by ambient temperature variation: A case-crossover study in Maputo, Mozambique. Clin. Neurol. Neurosurg. 2015, 129, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.M.; Dasenbrock, H.; Du, R. The association between meteorological parameters and aneurysmal subarachnoid hemorrhage: A nationwide analysis. PLoS ONE 2014, 9, e112961. [Google Scholar] [CrossRef] [PubMed]
- Lejeune, J.P.; Vinchon, M.; Amouyel, P.; Escartin, T.; Escartin, D.; Christiaens, J.L. Association of occurrence of aneurysmal bleeding with meteorologic variations in the north of France. Stroke 1994, 25, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Ishikawa, S.; Kajii, E. Cumulative effects of weather on stroke incidence: A multi-community cohort study in japan. J. Epidemiol. 2010, 20, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Nakaguchi, H.; Matsuno, A.; Teraoka, A. Prediction of the incidence of spontaneous intracerebral hemorrhage from meteorological data. Int. J. Biometeorol. 2008, 52, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Shinkawa, A.; Ueda, K.; Hasuo, Y.; Kiyohara, Y.; Fujishima, M. Seasonal variation in stroke incidence in Hisayama, Japan. Stroke 1990, 21, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Sobel, E.; Zhang, Z.X.; Alter, M.; Lai, S.M.; Davanipour, Z.; Friday, G.; McCoy, R.; Isack, T.; Levitt, L. Stroke in the Lehigh Valley: Seasonal variation in incidence rates. Stroke 1987, 18, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Tsementzis, S.A.; Kennet, R.P.; Hitchcock, E.R.; Gill, J.S.; Beevers, D.G. Seasonal variation of cerebrovascular diseases. Acta Neurochir. 1991, 111, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Oyoshi, T.; Nakayama, M.; Kuratsu, J. Relationship between aneurysmal subarachnoid hemorrhage and climatic conditions in the subtropical region, Amami-oshima, in Japan. Neurol. Med. Chir. 1999, 39, 585–590. [Google Scholar] [CrossRef]
- Buijs, J.E.; Uyttenboogaart, M.; Brouns, R.; de Keyser, J.; Kamphuisen, P.W.; Luijckx, G.J. The effect of age and sex on clinical outcome after intravenous recombinant tissue plasminogen activator treatment in patients with acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2015, 25, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Gokhale, S.; Caplan, L.R.; James, M.L. Sex differences in incidence, pathophysiology, and outcome of primary intracerebral hemorrhage. Stroke 2015, 46, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Rakers, F.; Schiffner, R.; Rupprecht, S.; Brandstädt, A.; Witte, O.W.; Walther, M.; Schlattmann, P. Rapid weather changes are associated with increased ischemic stroke risk: A case-crossover study. Eur. J. Epidemiol. 2015, 31, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, A.; Hajat, S.; Kovats, R.S.; Bisanti, L.; Rognoni, M.; Russo, A.; Paldy, A. An ecological time-series study of heat-related mortality in three European cities. Environ. Health 2008, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Su, H. Effects of climatic temperature stress on cardiovascular diseases. Eur. J. Intern. Med. 2010, 21, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Abboud, F.M.; Harwani, S.C.; Chapleau, M.W. Autonomic neural regulation of the immune system: Implications for hypertension and cardiovascular disease. Hypertension 2012, 59, 755–762. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Paper ID | Author and Year of Publication | Title | Country & City/Region | Latitude | Year(s) of Study | Sample Size | Age (Mean, Year) Female (%) | Only First-Ever Stroke | Stroke Subtype | Study Type | Study Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Abe 2008 [29] | Effects of meteorological factors on the onset of subarachnoid hemorrhage: a time-series analysis | Japan, Tokyo | 35.6833° N | 2005 | 1729 | 63.3 Female (60%) | No | SAH | Population study | ACDEF |
| 2 | Dawson 2008 [30] | Associations between meteorological variables and acute stroke hospital admissions in the west of Scotland | United Kingdom, Glasgow | 55.8580° N | 1990–2005 | 6389 | 71.2 Female (53%) | No | IS and ICH | Stroke registry | ACDE |
| 3 | Feigin 2000 [25] | A population-based study of the associations of stroke occurrence with weather parameters in Siberia, Russia (1982–1992) | Russia, Siberia | 61.0137° N | 1982–1992 | 2208 | Age range: 25–74 Female (57%) | Yes | IS, ICH and SAH | Stroke registry | ABCEF |
| 4 | Jimenez-Conde 2008 [17] | Weather as a trigger of stroke: daily meteorological factors and incidence of stroke subtypes | Spain, Barcelona | 41.3833° N | 2001–2003 | 1286 | Not reported | No | IS and ICH | Population | ABDE |
| 5 | Lee 2008 [31] | Seasonal variation in ischemic stroke incidence and association with climate, a six-year population-based study | China, Taiwan | 25.0330° N | 1998–2003 | 168,977 | Age range: 20–84 | No | IS | Population | AE |
| 6 | Magalhaes 2011 [32] | Are stroke occurrence and outcome related to weather parameters? Results from a population-based study in Northern Portugal | Portugal, Porto | 41.1621° N | 1998–2000 | 462 | All ages Female (62%) | Yes | IS and ICH | Stroke registry | ACDEF |
| 7 | Morabito 2011 [33] | Innovative approaches helpful to enhance knowledge on weather-related stroke events over a wide geographical area and a large population | Italy, Tuscany | 43.3500° N | 1997–2007 | 112,870 | All ages | No | IS, ICH and SAH | Hospital registry | ACDE |
| 8 | Han 2015 [34] | Effect of seasonal and monthly variation in weather and air pollution factors on stroke incidence in Seoul, Korea | South Korea, Seoul | 37.5667° N | 2004–2013 | 3001 | Age >19 Female (49%) | No | IS and ICH | Stroke registry | ACDEF |
| 9 | Chen 1995 [16] | Weather and stroke in a subtropical area: Ilan, Taiwan | Taiwan, Ilan | 24.7570° N | 1991 | 517 | All ages Female (39%) | No | IS, ICH and SAH | Population | ACDE |
| 10 | Fang 2012 [19] | Ambient temperature and spontaneous intracerebral haemorrhage: a crossectional analysis in Tainan, Taiwan | China, Taiwan | 22.9999° N | 08/2006–07/2008 | 933 | 62 Female (39%) | No | ICH | Stroke registry | ACDEF |
| 11 | Gomes 2014 [35] | Triggering of stroke by ambient temperature variation: a case-crossover study in Maputo, Mozambique | Maputo, Mozambique | 25.9500° S | 08/2005–07/2006 | 593 | 58.8 Female (48%) | Yes | IS and ICH | Population | ABDE |
| 12 | Lai 2014 [36] | The association between meteorological parameters and aneurysmal subarachnoid hemorrhage: a nationwide analysis | USA, 41 states | 38.8833° N | 2001–2010 | 16,970 | Median: 53 (IQR 34–72) | No | SAH | Population | ADE |
| 13 | Lejeune 1994 [37] | Association of occurrence of aneurysmal bleeding with meteorological variations in the north of france | France, North France region | 47.0000° N | 1989–1991 | 283 | 49.1 Female (53%) | No | SAH | Community | ABE |
| 14 | Matsumoto 2010 [38] | Cumulative effects of weather on stroke incidence: a multi-community cohort study in Japan | Japan, 12 communities | 35.6833° N | 04/1992–07/2002 | 450 | Age ≥30 in 1 community, 40–69 in 11 communities | Yes | IS, ICH and SAH | Population | ABDEF |
| 15 | Nakaguchi 2008 [39] | Prediction of the incidence of spontaneous intracerebral hemorrhage from meteorological data | Japan Shin-ichi | 34.3319° N | 01/2001–12/2003 | 164 | All ages | No | ICH | Community | ADE |
| 16 | Shinkawa 1990 [40] | Seasonal variation in stroke incidence in Hisayama, Japan | Japan, Hisayama | 33.6468° N | 11/1961–10/1985 | 308 | Age ≥40, 74 Female (49%) | Yes | IS, ICH and SAH | Population | ABCDEF |
| 17 | Sobel 1987 [41] | Stroke in the Lehigh Valley: seasonal variation in incidence rates | United States, Lehigh Valley | 40.6646° N | 07/1982–12/1983 | 1944 | All ages Female (51%) | No | IS, ICH and SAH | Hospital registry | ABCE |
| 18 | Tsementzis 1991 [42] | Seasonal variation of cerebrovascular diseases | United Kingdom, West Midlands Region | 52.489471° N | 1973–1980 | 12,262 | All ages Female (53%) | No | IS, ICH and SAH | Hospital registry | AE |
| 19 | Wang 2009 [15] | Temperature variation and emergency hospital admissions for stroke in Brisbane, Australia, 1996-2005 | Australia, Brisbane | 27.4667° S | 1996–2005 | 12387 | All ages | No | IS and ICH | Population | ACE |
| 20 | Oyoshi 1999 [43] | Relationship between aneurysmal subarachnoid hemorrhage and climatic conditions in the subtropical region, Amami-Oshima, in Japan | Japan, Amami-Oshima | 28.2500° N | 1986–1996 | 210 | All ages, 64.3 | No | SAH | Hospital registry | AE |
| 21 | Goggins 2012 [23] | Weather, season, and daily stroke admissions in Hong Kong | China, Hong Kong | 22.2783° N | 1999-–2006 | 130,962 | ≥35 | No | IS, ICH and SAH | Hospital registry | ACDE |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Cao, Y.; Hong, D.; Zheng, D.; Richtering, S.; Sandset, E.C.; Leong, T.H.; Arima, H.; Islam, S.; Salam, A.; et al. Ambient Temperature and Stroke Occurrence: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2016, 13, 698. https://doi.org/10.3390/ijerph13070698
Wang X, Cao Y, Hong D, Zheng D, Richtering S, Sandset EC, Leong TH, Arima H, Islam S, Salam A, et al. Ambient Temperature and Stroke Occurrence: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2016; 13(7):698. https://doi.org/10.3390/ijerph13070698
Chicago/Turabian StyleWang, Xia, Yongjun Cao, Daqing Hong, Danni Zheng, Sarah Richtering, Else Charlotte Sandset, Tzen Hugh Leong, Hisatomi Arima, Shariful Islam, Abdul Salam, and et al. 2016. "Ambient Temperature and Stroke Occurrence: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 13, no. 7: 698. https://doi.org/10.3390/ijerph13070698