
Abstract
Background
Individuals ≥80 years of age represent an increasing proportion of colon cancer diagnoses. Selecting these patients for elective surgery is challenging because of diminished overall health, functional decline, and limited data to guide decisions. The objective was to identify overall health measures that are predictive of poor survival after elective surgery in these oldest-old colon cancer patients.
Methods
Medicare beneficiaries ≥80 years who underwent elective colectomy for stage I–III colon cancer from 1992–2005 were identified from the Surveillance, Epidemiology and End Results(SEER)-Medicare database. Kaplan–Meier survival analysis determined 90-day and 1-year overall survival. Multivariable logistic regression assessed factors associated with short-term postoperative survival.
Results
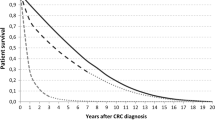
Overall survival for the 12,979 oldest-old patients undergoing elective colectomy for colon cancer was 93.4 and 85.7 %, at 90 days and 1 year. Older age, male gender, frailty, increased hospitalizations in prior year, and dementia were most strongly associated with decreased survival. In addition, AJCC stage III (vs stage I) disease and widowed (vs married) were highly associated with decreased survival at 1 year. Although only 4.4 % of patients were considered frail, this had the strongest association with mortality, with an odds ratio of 8.4 (95 % confidence interval, 6.4–11.1).
Conclusions
Although most oldest-old colon cancer patients do well after elective colectomy, a significant proportion (6.6 %) die by postoperative day 90 and frailty is the strongest predictor. The ability to identify frailty through billing claims is intriguing and suggests the potential to prospectively identify, through the electronic medical record, patients at highest risk of decreased survival.


Similar content being viewed by others

References
Werner CA. The Older Population: 2010. 2010. Available: http://www.census.gov/prod/cen2010/briefs/c2010br-09.pdf. Accessed March 22, 2012.
Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Waldron W, et al. SEER Cancer Statistics Review, 1975–2008, based on November 2010 SEER data submission, posted to the SEER web site, 2011. Available: http://seer.cancer.gov/csr/1975_2008/ Accessed June 5, 2011.
Hutchins LF, Unger JM, Crowley JJ, Coltman CA, Jr., Albain KS. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. New Engl J Med. 1999;341:2061–7.
Pope AM, Tarlov AR. Disability in America: Toward a National Agenda for Prevention. Washington, DC: The National Academy Press, 1991.
Robinson TN, Wu DS, Stiegmann GV, Moss M. Frailty predicts increased hospital and six-month healthcare cost following colorectal surgery in older adults. Am J Surg. 2011;202:511–4.
Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210:901–8.
Dasgupta M, Rolfson DB, Stolee P, Borrie MJ, Speechley M. Frailty is associated with postoperative complications in older adults with medical problems. Arch Gerontol Geriatr. 2009;48:78–83.
Saxton A, Velanovich V. Preoperative frailty and quality of life as predictors of postoperative complications. Ann Surg. 2011;253:1223–9.
Kristjansson SR, Nesbakken A, Jordhoy MS, Skovlund E, Audisio RA, Johannessen HO, et al. Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol. 2010;76:208–17.
Robinson TN, Wallace JI, Wu DS, Wiktor A, Pointer LF, Pfister SM, et al. Accumulated frailty characteristics predict postoperative discharge institutionalization in the geriatric patient. J Am Coll Surg. 2011;213:37–42; discussion 42–4.
Robinson TN, Eiseman B, Wallace JI, Church SD, McFann KK, Pfister SM, et al. Redefining geriatric preoperative assessment using frailty, disability and co-morbidity. Ann Surg. 2009;250:449–55.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56.
Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci. 2007;62:722–7.
Kunitake H, Zingmond DS, Ryoo J, Ko CY. Caring for octogenarian and nonagenarian patients with colorectal cancer: what should our standards and expectations be? Dis Colon Rectum. 2010;53:735–43.
Clark AJ, Stockton D, Elder A, Wilson RG, Dunlop MG. Assessment of outcomes after colorectal cancer resection in the elderly as a rationale for screening and early detection. Br J Surg. 2004;91:1345–51.
Hessman O, Bergkvist L, Strom S. Colorectal cancer in patients over 75 years of age—determinants of outcome. Eur J Surg Oncol. 1997;23:13–9.
Heriot AG, Tekkis PP, Smith JJ, Cohen CR, Montgomery A, Audisio RA, et al. Prediction of postoperative mortality in elderly patients with colorectal cancer. Dis Colon Rectum. 2006;49:816–24.
Greenblatt DY, Weber SM, O’Connor ES, LoConte NK, Liou JI, Smith MA. Readmission after colectomy for cancer predicts one-year mortality. Ann Surg. 2010;251:659–69.
O’Connor ES, Greenblatt DY, LoConte NK, Gangnon RE, Liou JI, Heise CP, et al. Adjuvant chemotherapy for stage II colon cancer with poor prognostic features. J Clin Oncol. 2011;29:3381–8.
Weiss JM, Pfau PR, O’Connor ES, King J, LoConte N, Kennedy G, et al. Mortality by stage for right- versus left-sided colon cancer: analysis of surveillance, epidemiology, and end results—Medicare data. J Clin Oncol. 2011;29:4401–9.
Potosky AL, Riley GF, Lubitz JD, Mentnech RM, Kessler LG. Potential for cancer related health services research using a linked Medicare-tumor registry database. Med Care. 1993;31:732–48.
Warren JL, Klabunde CN, Schrag D, Bach PB, Riley GF. Overview of the SEER-Medicare data: content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40:IV-3–18.
Bradley CJ, Given CW, Dahman B, Fitzgerald TL. Adjuvant chemotherapy after resection in elderly Medicare and Medicaid patients with colon cancer. Arch Intern Med. 2008;168:521–9.
Dobie SA, Baldwin LM, Dominitz JA, Matthews B, Billingsley K, Barlow W. Completion of therapy by Medicare patients with stage III colon cancer. J Natl Cancer Inst. 2006;98:610–9.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
Taylor DH, Jr., Ostbye T, Langa KM, Weir D, Plassman BL. The accuracy of Medicare claims as an epidemiological tool: the case of dementia revisited. J Alzheimers Dis. 2009;17:807–15.
Lieberman R, Abrams C, Weiner JP. Development and Evaluation of the Johns Hopkins University Risk Adjustment Models for Medicare + Choice Plan Payment. Baltimore, MD: Centers for Medicare and Medicaid Services, U.S. Department of Health and Human Services; 2003.
Neuman H, O’Connor ES, Weiss J, LoConte NK, Greenblatt DY, Smith MA. Surgical treatment of colon cancer in patients older than 80 years of age. J Clin Oncol. 2011;29:6071.
Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing. 2006;35:526–9.
Steverink N, Slaets JPJ, Schuurmans H, Lis van M. Measuring frailty. development and testing of the Groningen Frailty Indicator (GFI). Gerontologist. 2001;41:236–7.
Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. J Gerontol A Biol Sci Med Sci. 2007;62:738–43.
Dimick JB, Osborne NH, Hall BL, Ko CY, Birkmeyer JD. Risk adjustment for comparing hospital quality with surgery: how many variables are needed? J Am Coll Surg. 2010;210:503–8.
Reuben DB. Medical care for the final years of life: “When you’re 83, it’s not going to be 20 years”. JAMA. 2009;302:2686–94.
O’Donnell S, Cranney A, Jacobsen MJ, Graham ID, O’Connor AM, Tugwell P. Understanding and overcoming the barriers of implementing patient decision aids in clinical practice. J Eval Clin Pract. 2006;12:174–81.
Caldon LJ, Collins KA, Reed MW, Sivell S, Austoker J, Clements AM, et al. Clinicians’ concerns about decision support interventions for patients facing breast cancer surgery options: understanding the challenge of implementing shared decision-making. Health Expect. 2011;14:133–46.
Conley DM, Singer SJ, Edmondson L, Berry WR, Gawande AA. Effective surgical safety checklist implementation. J Am Coll Surg. 2011;212:873–9.
Acknowledgment
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the Applied Research Program, NCI; the Office of Research, Development and Information, CMS; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database. The collection of the California cancer incidence data used in this study was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract N01-PC-35136 awarded to the Northern California Cancer Center, contract N01-PC-35139 awarded to the University of Southern California, and contract N02-PC-15105 awarded to the Public Health Institute; and the Centers for Disease Control and Prevention’s National Program of Cancer Registries, under agreement No. U55/CCR921930-02 awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and endorsement by the State of California, Department of Public Health the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors is not intended nor should be inferred. The authors acknowledge the efforts of the Applied Research Program, NCI; the Office of Research, Development and Information, CMS; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database. Support for this project was provided by the Health Innovation Program and the Community-Academic Partnerships core of the University of Wisconsin Institute for Clinical and Translational Research (UW ICTR), grant 1UL1RR025011 from the Clinical and Translational Science Award program of the National Center for Research Resources, National Institutes of Health and by the University of Wisconsin Carbone Cancer Center, grant P30CA014520-34 from the National Cancer Institute, National Institutes of Health. Additional funding for this project was provided by the UW School of Medicine and Public Health from The Wisconsin Partnership Program.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Neuman, H.B., Weiss, J.M., Leverson, G. et al. Predictors of Short-Term Postoperative Survival After Elective Colectomy in Colon Cancer Patients ≥80 Years of Age. Ann Surg Oncol 20, 1427–1435 (2013). https://doi.org/10.1245/s10434-012-2721-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2721-8