Article Text

Abstract
Objective To assess the prevalence of engagement in self-asphyxial (risk-taking) behaviour (SAB) (‘choking game’) and associated morbidity and mortality in children and young people up to age 20.
Design Systematic literature review.
Search strategy Electronic database search of MEDLINE, Embase, PsycINFO, CINAHL, PubMed, Web of Science Core Collection, BIOSIS citation index and the Cochrane register with no language or date limits applied. References of key papers were reviewed, and experts were contacted to identify additional relevant papers.
Eligibility criteria Systematic reviews, cross-sectional, cohort and case–control studies, and case reports examining SAB with regard to individuals aged 0–20 years, without explicitly stated autoerotic, suicidal or self-harm intentions were included.
Results Thirty-six relevant studies were identified, and SAB was reported in 10 countries. In North America, France and Colombia, awareness of SAB ranged from 36% to 91% across studies/settings, and the median lifetime prevalence of engagement in SAB was 7.4%. Six studies identified the potential for SAB to be associated with engagement in other risk behaviours. Ninety-nine fatal cases were reported. Of the 24 cases described in detail, most occurred when individuals engaged in SAB alone and used a ligature.
Conclusions The current evidence on SAB among young people is limited, and stems predominantly from North America and France. Awareness of SAB among young people is high, and engagement varies by setting. Further research is needed to understand the level of risk and harm associated with SAB, and to determine the appropriate public health response.
- Injury Prevention
- Adolescent Health
- School Health
- Public Health
- Paediatric Practice
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Engagement of young people in self-asphyxial behaviour (SAB) is dangerous, and can be fatal.
Young people engage in SAB in groups with their friends, but some continue the practice on their own.
Despite SAB being around for decades, there is limited and little consistent evidence about the prevalence, associated risk factors and levels of morbidity and mortality associated with engagement in SAB.
What this study adds?
The median lifetime prevalence rate of ever engagement in SAB in young people is 7.4% in the included cross-sectional studies from North America, France and Colombia.
Fatal cases due to SAB have been formally reported in 10 countries around the world. Most fatal cases seem to occur when individuals engage in SAB on their own, and use ligaments to engage in the practice.
Individuals engaging in other risk behaviours were seen to be more likely to engage in SAB, which is in line with the literature on multiple risk behaviours, which are shown to cluster and co-occur in adolescence.
Introduction
Adolescence is a period of increased susceptibility for engaging in a range of risk behaviours such as binge drinking, unprotected sex and recreational drug use.1 ,2 One less well-reported and researched form of risk behaviour in young people is engagement in self-asphyxial behaviour (SAB),3 also known as the ‘choking game’.4–7 SAB is defined as ‘self-strangulation or strangulation by another person with the hands or a noose to achieve a brief euphoric state caused by cerebral hypoxia’.8 A variety of methods are used to achieve the state of unconsciousness, including hyperventilation, strangulation, chest and neck compression or ligatures such as ropes or scarves.9–13 Various negative short-term and long-term health outcomes from engagement in SAB have been reported, including chronic headaches, confusion, amnesia, neurological damage and death.14–17
Engagement in SAB is not a new phenomenon. It was reported in the British Medical Journal in 1951,18 and similar sorts of activities are known internationally.15 ,19–23 SAB is mainly referred to as the ‘choking game’ in the literature despite the existence of an extensive list of other culture-specific and language-specific terms (see online supplementary file A). The main motives for engagement in SAB are reported to be fitting in with a social group, thrill-seeking and experimentation.24 ,25 These are argued to be distinctly different from self-harm, suicidal intentions and sexual asphyxia also known as autoerotic asphyxiation.10 ,17 ,26
Despite SAB being documented in the medical literature, limited epidemiological data are available on the prevalence of SAB and associated risk behaviours. Prevalence estimates are mainly from cross-sectional surveys undertaken in North America, and vary in their findings.27–30 The literature reports on a limited number of fatal cases due to SAB; however, advocacy groups suggest that the number of fatalities is more than 1000 worldwide.31 ,32
To our knowledge, there have been no comprehensive reviews of the evidence to assess the prevalence and associated risk factors of engagement in SAB in young people. The only review we are aware of compared the clinical and psychopathological data of SAB with sexual asphyxia.17 It includes limited information on the frequency and associated risk behaviours of SAB.
The objective of the present review is to systematically assess the prevalence of awareness, engagement, associated morbidity and mortality in SAB in young people aged 0–20 years. We conducted the review in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA).33
Methods
Search strategy
A systematic search was carried out in July 2014 using a predefined search protocol registered on the PROSPERO database.34 Neither date nor language restrictions were applied. The following eight databases were searched: MEDLINE, Embase and PsycINFO, CINAHL, PubMed, Web of Science Core Collection, BIOSIS citation index and the Cochrane Library. The search strategy was tested for effective retrieval of key papers prior to the actual search (see online supplementary file A).
All titles and abstracts retrieved through the searches were saved using EndNote X7 reference manager software. Duplicates were removed. Titles, abstracts and full-text references were screened for inclusion by one author with a random subset of 10% screened by a second author at each stage. Inter-rater reliability scores were calculated using Cohen's kappa, and a high level of agreement was found at all stages (figure 1). Discrepancies between reviewers were resolved by discussion.

PRISMA flow chart of study search and selection process. PRISMA, Preferred Reporting Items of Systematic Reviews and Meta-Analyses; SAB, self-asphyxial behaviour.
In addition to the database search, 13 experts in the field were contacted and reference lists of 23 key SAB publications, two known SAB websites (http://www.jeudufoulard.com/ and http://www.rememberingcolin.com), and all included cross-sectional studies were hand-searched and screened to identify additional relevant studies.
Eligibility criteria
To be considered for inclusion in the review, studies had to be either systematic reviews or provide original data on young people's engagement in SAB with the intention of undertaking an activity or a game. Any methods and settings of engagement in SAB were eligible for inclusion. Studies, where the intention to engage in SAB was described as autoerotic, or for self-harming with or without suicidal intent, were excluded.
The focus was on studies of children and young people aged 0–20 years. The age cut-off for relevant cases was 20 years, and no lower age limit was applied.24 ,35–37
Data extraction
Included studies were categorised by study design. Data extraction was carried out using predesigned data extraction forms for each study design. Data were extracted on the key study characteristics, design, methods of data collection, participant characteristics, results and conclusions drawn by authors.
Quality assessment
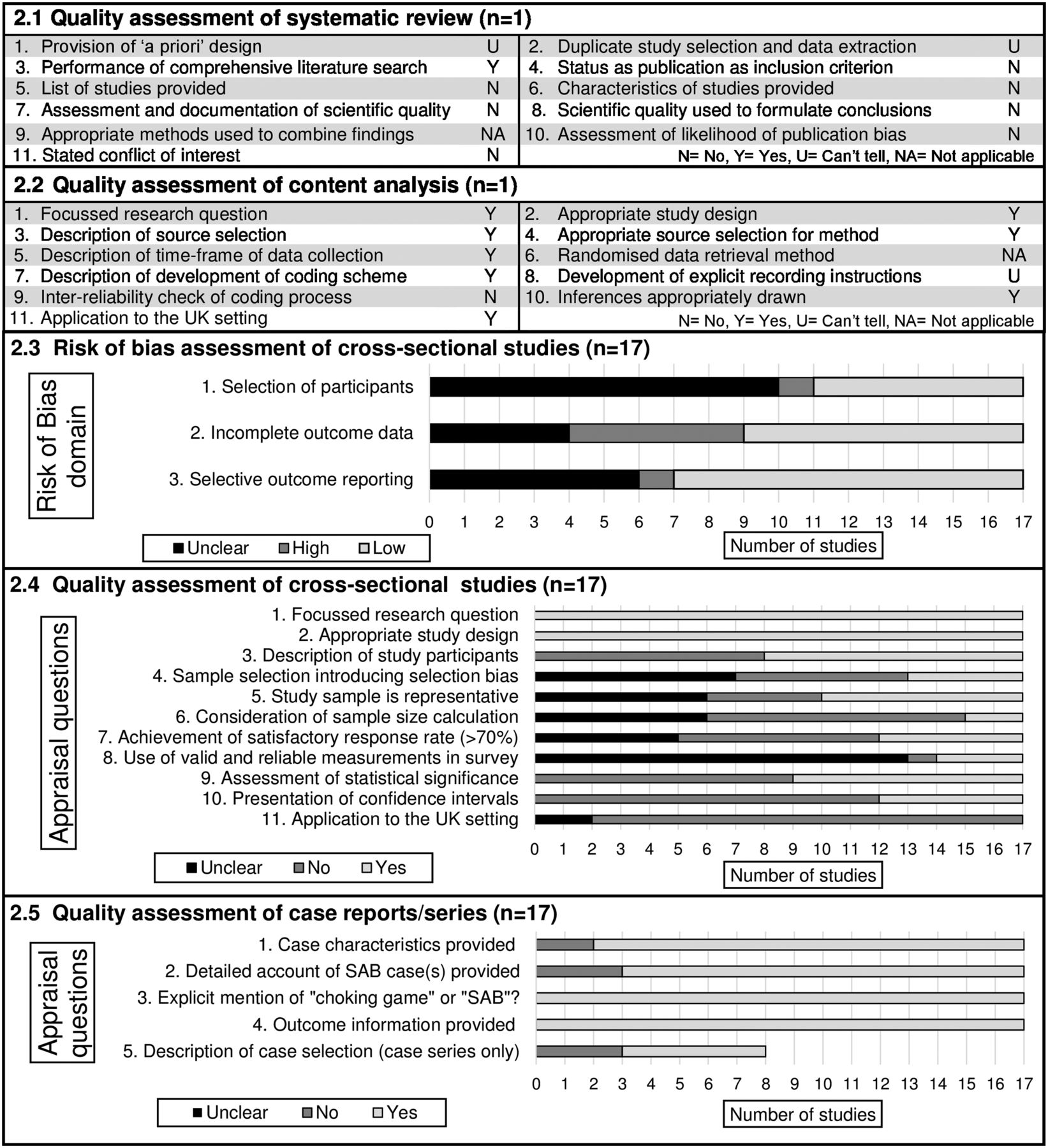
Alongside the data extraction, two reviewers assessed the quality using a predetermined assessment form (available from authors). Systematic reviews were quality appraised using A MeaSurement Tool to Assess systematic Reviews (AMSTAR).38 To assess the quality of content analysis studies, authors created 11 appraisal questions based on the literature on content analysis and an adaptation of Crombie's critical appraisal guide.39–41 The quality appraisal of cross-sectional studies was based on an adaptation of the Risk of Bias Assessment Tool for Nonrandomized Studies42 and Crombie's critical appraisal guide.39 Quality appraisal of case studies and case series was based on a short array of questions informed by the Strengthening the Reporting of Observational Studies in Epidemiology statement.43
Results
The search yielded 11 024 results, relating to 6953 different papers after the removal of duplicates, of which 164 references were assessed in full-text (see figure 1). Thirty-six references were included: 1 systematic review, 1 content analysis, 16 cross-sectional studies, 17 case reports/series and 1 study providing both cross-sectional and case-series data (see online supplementary file B). Almost two-thirds of studies were conducted in the USA or Canada. We found substantial heterogeneity in the studies, and therefore, decided to conduct a narrative analysis.
Quality of studies
A summary of quality assessment results is presented in figure 2. The systematic review was of uncertain quality as limited information was provided on its methodology; the content analysis was of high quality as methods of source selection and coding were thoroughly described. Only four cross-sectional studies were considered to be of good overall quality,28–30 ,36 and many studies lacked detail on their methodology. The majority of case reports/series included sufficient details of the demographics, settings and clinical findings of the reported cases. No studies were excluded based on their quality in order to provide an overview of all the literature on SAB.
{kind=link}
{kind=link}
Findings from quality assessment of included studies. SAB, self-asphyxial behaviour.
Systematic review
The systematic review17 assessed and compared the clinical and psychopathological features of SAB and erotic asphyxiation in studies published between 1988 and 2011. The review included 17 references on SAB, four of which refer to original studies, which are also included in the present review. Authors suggest that SAB and erotic asphyxiation can carry addictive properties, and advise clinicians to educate themselves on the characteristics and warning signs of these behaviours.17
Content analysis
One relevant content analysis was identified;12 it investigated videos showing recreational partial asphyxiation published in the video-sharing website YouTube in 2007. Sixty-five SAB videos were included with 110 participants (90% male) of estimated age between 12 and 18 years and of mixed ethnicity. Hypoxic seizures were seen in over half (55%) the videos.12
Cross-sectional studies
Seventeen cross-sectional studies were included. These studies were conducted between 2007 and 2012 in four countries: US A (n=9), France (n=4), Canada (n=3) and Colombia (n=1) (table 1). Nine surveys were part of a general school health assessment, and seven aimed to obtain in-depth knowledge about SAB. The majority used self-report questionnaires, and one conducted interviews.45 Participants were predominantly aged 12–17, and response rates ranged from 62.2%46 to 95.6%.28
Cross-sectional studies: data collection and survey details
The lifetime prevalence of engaging in SAB ranged from 6% to 16% in France, 5.3%–7.4% in Canada and 3.8%–17.1% in the USA (table 2). The only Colombian study reported a prevalence of 54%.48 The median lifetime prevalence rate based on all available prevalence rates is 7.4%. Current participation was below 5% in most studies.44 ,46 When asking young people about their knowledge of others’ engagement in SAB, prevalence rates ranged from 18.8%52 to 45%.30 Awareness of SAB ranged from 36.2%36 to 72%.48 Individuals reported first engaging in SAB when they were around 8–15 years of age,30 ,44 and mentioned that they have come into contact with SAB primarily through their friends at school.48 ,50
Cross-sectional studies: SAB awareness and engagement
Studies generally reported that engagement in SAB is a group activity.30 ,50 However, a minority of young people also reported solitary engagement in SAB, without another person present. Studies revealed that 11%30 ,50–23%44 of young people who engaged in SAB did so without others present, and two studies reported the prevalence of solitary engagement in the respective total sample of students to range from 0.5%52 to 1.5%.44 SAB was reported to take place in a range of settings44 ,45 ,48 ,50 and for various reasons44 ,45 ,48 ,50 (see online supplementary file C).
When asked, young people mentioned having observed or experienced various negative health outcomes as consequences of engagement in SAB. These included having experienced headaches and dizziness,48 and having seen others become unconscious.50 Despite reporting on negative consequences of engagement in SAB, a substantial proportion of young people (17%–40%) thought that there were no risks involved.30 ,45 ,48
One study investigated the methods of prevention.30 Authors report that a majority of young people (57%) mentioned that knowing that SAB can lead to death or brain damage would make them stop, that younger children would most likely listen to their parents whereas older children reported to be most influenced by near-victims or peers.30
Risk factors for SAB
Six out of 17 studies3 ,28 ,29 ,36 ,44 ,46 reported the potential for other risk factors to be associated with engagement in SAB, and were conducted in France (n=2) and North America (n=4) (see online supplementary file D). Three of these were conducted as part of larger school surveys,3 ,28 ,36 and three were individual studies on SAB.29 ,44 ,46 Only two of the studies28 ,29 explicitly mentioned controlling their analysis for possible confounding variables whereas this was not clear in all other cases, and highlights that the following section will need to be interpreted with caution. Five studies reported associations between SAB and one of the following risk-behaviour domains: substance misuse, risky sexual behaviours, poor mental health, poor dietary behaviours or engagement in risky sports.3 ,28 ,29 ,36 ,44
No association was found with engagement in physical activity28 and having experienced accidents or hospital admissions.44 Previous experience of violence,28 ,29 being of a more impulsive and thrill-seeking personality44 ,46 and lower school achievement28 ,29 ,44 were further linked to an increased likelihood of engagement in SAB. Mixed evidence was obtained with regard to gender, age and living situation.
Case reports/series
Eighteen relevant references were included that referred to case descriptions of young people engaged in SAB (table 3). One hundred and eighty SAB cases, 99 of which were fatal, were reported in 10 of the 11 countries.
Two key case reviews were conducted in the USA8 and Canada.64 Toblin et al8 undertook a retrospective newspaper analysis to estimate the national incidence of deaths resulting from SAB among young people under 20 years of age between 1995 and 2007. Authors reported 82 probable SAB cases, 87% of which were males with a mean age of 13.3 years (range 6–19 years). Among 70 cases where sufficient detail was reported, 95% of cases engaged in SAB without others present. Further, most parents (93%) were not aware of SAB until their child's death.8 McFaull64 searched the Canadian injury surveillance system in 2006 in order to identify cases of asphyxia in young people, and identified 74 cases, 72% of which were males with a median age of 12.1 years (range 4–17 years). Seven cases involved solitary strangulation in which injury occurred, and one fatal case was reported.64
Fifteen case reports described SAB cases in sufficient detail to highlight possible risk factors for SAB (see online supplementary file E). The mean age of these 24 cases was 12.5 years (range 9–20 years), 83.3% (n=20) were male and 58% (n=14) of cases resulted in death. All of the fatal cases involved the use of ligatures, and most occurred when the individual was alone. Settings in which SAB took place were varied and included the school and home. Some fatal cases were only determined to be caused by SAB after discussions with friends or family members8 ,55 ,60 or after reviewing media content, such as from emails or phones.55 ,65
Discussion
Main findings of this study
Thirty-six studies, the majority of which were cross-sectional and case series, were included in the review. SAB has been reported in 10 countries. The median lifetime prevalence of engagement in SAB was 7.4%. Six studies identified the potential for SAB to be associated with engagement in other risk behaviours, which is in line with the literature on multiple risk behaviours, which are shown to cluster in adolescence and to carry similar risk and protective factors.66 ,67 Whereas SAB engagement usually occurs as a group activity, some individuals engage in SAB on their own. The prevalence of SAB engagement among young people varied widely, which suggests that SAB might cluster in certain areas and environments. There is potential for SAB engagement to spread to other areas, particularly through the use of social media, which is widely adopted by young people.68 Differences in prevalence estimates may also reflect different study methodologies. Similarly, awareness levels differ among young people as well as among parents and physicians.23 ,69
Three cross-sectional studies were excluded as the mean age of respondents was above 20 years.35 ,70 ,71 Similar to included studies, lifetime prevalence in these studies were 4%35 and 16.2%.71
Strengths and limitations
A strength of the review is the comprehensive search strategy, which included unpublished, grey literature to minimise publication bias. However, there may be further grey literature, which was not retrieved. Our inclusion of unpublished reports inevitably means that the quality of the studies is mixed.
A variety of descriptions of SAB were used in studies, which highlights the lack of an overall definition.4 ,5 ,29 As detailed in the quality assessment, some cross-sectional studies included non-random samples, had low response rates and used a single question to assess SAB engagement. These limitations require careful data interpretation and limit the generalisability of studies to other settings and countries. Additionally, caution needs to be taken in the assessment and interpretation of risk factors for engagement. Moreover, asphyxia cases reported in newspaper articles or media searches were acknowledged by authors to have low sensitivity and specificity;8 ,12 a high proportion of reported cases might be due to other causes (eg, suicide), so estimates of the number of deaths from SAB should be interpreted with caution.
Some of the studies excluded from the review described SAB-type methods and behaviours in young people without explicitly naming this as SAB;72 this coupled with the fact that many fatal cases were only retrospectively linked to SAB11 ,55 ,60 highlights that there is a lack of knowledge and understanding about SAB and a risk for misclassification of cases.16 ,21 ,55 ,61 It has been suggested that: ‘… what we are seeing in terms of children dying is only the tip of the iceberg of a major problem which to a large extent is unrecognised’.73
Preliminary data from the Office of National Statistics (ONS) on deaths of young people aged 11–15 years over a 10-year period (2002–2011) in England and Wales revealed that 145 deaths were categorised as ‘other accidental suffocation and strangulation’ (International classification of Diseases-10 (ICD-10) code W76), and 105 deaths were categorised as ‘hanging, strangulation and suffocation with undetermined intent’ (ICD-10 code Y20)74 (unpublished data). Some of these might have been due to SAB.
Recommendations and future research
As limited published epidemiological data exist of SAB, we recommend further research is undertaken, particularly in countries where cases have been reported, but where no formal research on the prevalence has yet been undertaken. A wide range of prevalence estimates was obtained, which might be due to the use of different definitions and explanations of SAB within questionnaires, different study methodologies, questionnaire designs and levels of awareness, culture and engagement in SAB. It would be valuable to investigate the roles played by these factors in future research to help find explanations for the range of estimates. Additional approaches, such as investigating potential deaths through existing databases, for example, the Child Death Overview Panels (CDOP) or the ONS data in England, and making use of qualitative studies on SAB, should be considered. Finlay and colleagues reported reviewed cases of death of young people hanging from bunk beds based on the CDOP data in England, and reported that 27 out of 62 deaths from strangulation were from bunk beds with the potential for some of these deaths to be due to the SAB.75 Additionally, various education and intervention programmes are available, but none of these have yet been formally evaluated.
Collaboration and increased learning about this behaviour across countries, particularly among professional groups in contact with young people, may lead to a better and more accurate understanding of SAB.16 ,60 Public health responses have emerged in some countries, but not in others.9 ,36 ,76
We consider it likely that specific intervention and prevention activities will need to be tailored to different settings. For areas in which SAB has been shown to be prevalent, current efforts are seen as inadequate.45 As it has been suggested that knowledge and identification of symptoms and signs of engagement in SAB could have possibly enabled early identification and possible prevention of fatal cases, we believe that clinicians, paediatricians, health professionals and teachers should receive education on the symptoms and signs of SAB.22 ,37 ,65 ,77 The need to educate health professionals has been highlighted as awareness of SAB will enable these individuals to identify symptoms and signs and to act as educators to young people and their parents.6 ,69 Discussions should include identifying who else would need to be educated about SAB, such as coroners, medical examiners, CDOP members, emergency service personnel and the police. We further recommend that more research is carried out together with young people to develop appropriate education material. In line with recommendations from others,12 ,76 ,78 we further recommend removing existing videos about SAB from the internet and ensuring that preventative website rather than promotional websites appear first on internet searches.12
Conclusions
SAB engagement has been reported in 10 countries with high levels of awareness in young people and various levels of actual engagement. SAB is a potentially dangerous activity, which can be fatal. Further research is needed to understand the level of risk and harm associated with SAB and to determine appropriate education and prevention approaches.
Acknowledgments
The authors would like to thank the reviewers for their helpful and constructive comments that contributed to improving the final version of the paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online supplement
- Data supplement 4 - Online supplement
- Data supplement 5 - Online supplement
Footnotes
Contributors RK, TH and DG originally conceived the idea for the systematic review. TH and HB wrote the protocol for this review, and specified the search strategy. HB and RK carried out the search, screening and identification of other references. HB undertook the data extraction for the review, and wrote a first draft of the review, which was then revised by RK, TH and DG.
Funding The work by RK and HB was undertaken with the support of The Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer), a UKCRC Public Health Research Centre of Excellence. Joint funding (MR/KO232331/1) from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the Welsh Government and the Wellcome Trust, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged. DG is a NIHR senior researcher. TH was funded by the Public Health Specialty Training Programme in the South West of England.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full search strategy for each database and the quality appraisal form are available from the authors on request.