
Abstract
Study design: Before and after investigation of the effects of a wheelchair ergometer Training programme.
Objective: To investigate the effects of an original interval-training programme on work capacity and cardiorespiratory variables with spinal cord-injured persons (SCIP's) on a wheelchair-specific ergometer.
Setting: BESANCON, FRANCE.
Methods: Seven SCIP's (male) performed 45 min of wheelchair ergometry three times per week, for 6 weeks. Training effects on maximal dynamic performance and endurance capacity were studied by comparison of performance and cardiorespiratory responses observed during both a maximal progressive test (10 W/2 min) and the same training session performed before and after training.
Results: Training induced significant improvements in maximal tolerated power (+19.6%), in peak oxygen consumption ( +16%), and in oxygen pulse (O2p,+18.7%).
At ventilatory threshold, significant improvements were also observed in power output (+63%), (+ 34.1), ventilation (+ 37.1%), and (+ 19.9% ). Heart rate and ventilation were significantly lower (−11 and −14.6%, respectively) after training at the same work rate, while was unchanged. Between the first and the last training session, the total physical work was improved by 24.7%, whereas heart rate was unchanged.
Conclusion: An interval-training programme individualised to each paraplegic subject using a wheelchair ergometer can significantly improve the fitness level and endurance capacity.
Similar content being viewed by others


Introduction
The loss of motor function by spinal cord injury may lead to a relatively sedentary lifestyle. A reduction in physical activity leads to deconditioning and to a decreased capacity for physical work. Furthermore, a spinal cord-injured person's (SCIP's) daily activities are not intense enough to prevent deterioration of their physical fitness.1 It was reported2 that cardiovascular and respiratory diseases3 were the leading cause of death among the spinal cord-injured (SCI) population. A lack of physical fitness for specific tasks can be a serious obstacle to autonomy and can lead to a loss of independency. This degenerative process may be reversible through exercise training.4 Nevertheless, few studies have attempted to define the exact guidelines of training following spinal cord injury.5,6
According to these studies, it is possible to propose recommendations for SCI population training such as using a wheelchair ergometer. This ergometer is less stressful than an arm ergometer7 and mimics closely the daily motor tasks of wheelchair users.
Minimal recommendations would require a training programme of 5 weeks,8,9,10 with 20-min sessions11,12,13,14,15 performed two times per week,6,15 at an intensity of 70% of the maximal heart rate (HR).16 Intermittent exercise intensities may be more beneficial since they mimic the intermittent nature of daily activity patterns.6
By applying all these considerations, it was decided to use the interval-training programme of Gimenez17,18,19 named Square Wave Endurance Exercise Test (SWEET) in order to prevent SCIPs from undergoing functional degeneration.
Materials and methods
Subjects
Seven male subjects (age=35±13 years (mean±SD), weight=72±11 kg and height=176±6 cm) participated in this study and gave their informed written consent.
All of them had been SCI for at least 1 year with a stable lesion level between T6 and L5. They were physically active without any specific upper-body training. According to the American Spinal Injury Association (ASIA) classification rules they were classified as ASIA A. Their characteristics are presented in Table 1. Our local ethical committee has approved this study.
Tests performed
Training effects were evaluated by comparison of the performance and cardiorespiratory responses recorded during a maximal progressive test and the same (work-rate) training session performed at the beginning and at the end of the conditioning programme.
In this case, the subjects repeated exactly the protocol of session number 2 and the cardiovascular variables during the final base and peak loads were compared after training to the responses recorded during session number 2.
All tests and sessions were performed at the same speed chosen by the patient, generally in the range of 1.39–1.67 m/s of linear displacement.
The progressive wheelchair test started with a rest period of 6 min on the wheelchair ergometer in order to stabilise the different cardiorespiratory variables. This was followed by a 2 min warm-up, which was performed at a residual friction power of 15 W. The load was then increased by 10 W every 2 min until the subject was no longer able to maintain the required speed. The highest load that could be maintained with a constant speed for 1 min was taken as the maximal tolerated power (MTP, watts). peak was determined as the highest recorded in a 30 s average.
Ventilatory threshold (VT) was assessed from respiratory variables according to Wasserman et al.20 Three observers determined the VT. The mean of the two closest values was determined as the VT. For each measured variable, the absolute value observed at the VT level was selected and expressed as a percentage of the peak value.
All tests, including the training session, were performed under medical supervision.
Training period
Subjects performed 45 min of wheelchair ergometry three times per week, for 6 weeks. Sessions consisted of nine successive work bouts of 5 min each. Each exercise bout consisted of a 4-min period of moderate exercise, named ‘base’ level, followed by a 1-min period of intense exercise, named ‘peak’ level. Initially, the base is set at a power output corresponding to the VT and the peak at the MTP obtained during the maximal test before training. The intensity of each training period was determined to lead up to almost 80% of maximal HR by the end of the ninth peak.
Throughout the training sessions, the peak and the base loads were alternately adjusted (+10 W) when the HR registered at the end of the ninth peak was at least 10 breaths (b)/min lower than the highest HR of the first training session. This adjustment was to assure a constant level of relative intensity throughout the training programme considering adaptations that occur with training over time.
Total physical work (TPW) during the SWEET was computed for each training session (1 W=1 J/s).17,21
Measurements
During each test, expired gases were sampled and analysed with a breath-by-breath gas analyser system (Medical Graphics type CPX/D, MSE, Strasbourg, France). The gas analyser system was calibrated before and after each test using gases of known concentrations. All ventilatory variables were averaged every 30 s.
The respiratory and metabolic parameters monitored included ventilation (VE, 1/min), respiratory rate (f, b/min), tidal volume (Vt, 1), oxygen uptake ( ml/min and ml/min/kg), and CO2 production ( ml/min). HR (b/min) was continuously monitored during each test and each training session by telemetry (PE 4000 sport tester, Polar, Finland). Respiratory exchange ratio /) and oxygen pulse (/HR, ml/b) were then calculated.
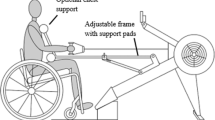
Both the training and tests were performed with the same ergometer (VP100H-HEF tecmachine, Andrezieux Boutheon, France) using the personal wheelchair of each subject (Figure 1). This ergometer22 has a single motorised roller with enslaved braking and an electromagnetic system. This system is controlled by specific software, which allows the subject to work at a required speed and to record the resulting torque. The calculation of this torque simultaneously takes into account, the actual braking force applied, the instantaneous speed of the roller, and the positive variation of the speed. During the exercise, the subject was able to see all the information concerning speed and power output via a control screen.

Wheelchair fixed on the ergometer used for the training and the testing sessions
Statistical analysis
All values are given as mean and standard deviation or extreme values, and are expressed in percent changes obtained after training. The delta percent (Δ%) changes are calculated as the mean of the individual variation ((value after training−value before training/value before training)100%). Training effects were analysed with Student's t-test. Statistical significance was set at the 0.05 level.
Results
Attendance of the volunteers at the training sessions was outstanding. All of our volunteers completed the training. The programme was perfectly tolerated by the subjects without excessive fatigue or shoulder pain.
Comparisons of peak values obtained during maximal incremental tests before and after training are presented in Table 2. Wheelchair training produced a significant increase in MTP (+19.6%), in peak (+16%), peak (+16.4%), and O2p (+18.7%). Peak HR and respiratory rate were unchanged after the training. Despite their magnitude, the changes in VE (+11.7%) and Vt (+11.9%) were not significantly different.
Table 3 presents the different responses corresponding to the VT level before and after training. A significant improvement in power output (+63%) associated with significant increases of physiological variables (+34.1%), (+49.9%), (+37.1%), and (+19.9%). Oxygen uptake observed at the VT level corresponds to 60.1 and 69.8% of the peak oxygen uptake before and after training, respectively.
During the same training session performed at the same loads before and after training (Table 4), a significantly lower HR was observed during the last base workload (−11.1%). There was also a significant difference at the last peak in O2 pulse (8.6 (7.3–11.3) versus 10.2 (9.4–12.1) ml/b) and in VE (52.3 (33–74.9) versus 47.8 (36.4-67.5) 1/min). Oxygen consumption was unchanged, as well as Vt and f.
These results expressed in percentage of the peak value obtained before and after showed significant differences in VE between the base (−27.6%) and the peak intensities (−28.5%), respectively, and in VO2 between the base intensities (−20.9%) (Table 4).
Between the first and the last training session, the TPW (1.9 (1.1–2.5) versus 2.4 (1.5–3.3) kJ/kg) was improved by 24.7% (P<0.01), whereas HR was unchanged at the base and at the peak, respectively.
Discussion
The SWEET concept has successfully been performed with able-bodied subjects.17,18,19,23 During the development of the SWEET protocol,17,18,19 work intensity at the base level was 50% MTP, and MTP at the peak level. With experience, recommendations required increasing the base level intensity to a level corresponding to VT while maintaining the peak level at MTP. This new version also showed beneficial results with patients suffering from chronic airway obstruction,21 after cardiac transplantation24,25 and with able-bodied subjects;23,26 however, it has never been performed with SCI patients. As such, the originality of this study is that the version of the SWEET with base intensity at VT and peak at MTP has never been proposed to paraplegic subjects with this wheelchair-specific ergometer and these work intensities.
Tordi et al27 proposed another version of the SWEET for paraplegics on a wheelchair ergometer. Their study used a base work intensity of 50% MTP, and a peak intensity of 80% MTP. The length of the programme was 4 weeks and a session duration of only 30 min. In this present study, patients had a higher and longer training period in which they realised a longer training period (6 weeks), longer exercise sessions (45 min), and with higher intensities (VT and peak). Owing to these differences, it was believed that the beneficial results obtained in this study should be greater than those of Tordi et al.27
Tordi et al27 obtained significant improvements in maximal values after training in MTP (+27.9%), in peak (+18.5%), peak (+15.9%), and O2p (+23.9%).
Between the first and the last training session, TPW improved by 32%. Such improvements were maybe because Tordi's subjects were less active than the subjects who participated in this study. Indeed, their subjects were newly injured, contrary to the patients in this study who were paraplegics for at least 1 year. It is generally accepted that if the patients are deconditioned at the beginning of the programme, improvements will be higher.
As expected and previously demonstrated in the literature,5 the results of the present study indicate that paraplegics can improve their physical work capacity by a programme of regular exercise. However, the main advantage of this training programme is related to its specifications and this could explain its efficiency.
Firstly, the ergometer used for training and testing has been specifically designed for use with one's personal wheelchair.22 It respects the characteristics of wheelchair propulsion and the wheelchair adjustment of each subject.
As such, the subjects were quickly accustomed to this type of exercise and optimised the time of training. Moreover, with the control screen, both the subject and the technician can continuously monitor the propulsion speed during the training session.
The specific software developed with the ergometer controlled the intensity and the duration of every session. Therefore, the training protocol concerning speed and power output was followed precisely. Secondly, the intensity specification of each session requires a high level of the endurance capacity of the subject.
This was confirmed by the responses observed at the end of the first training session, where and HR represented approximately 68% of the maximal value registered during the previous MPT (Table 4). The HR monitoring and control for each training session by load readjustment enabled the subject to respect the intensity recommendations throughout the entire training period (Table 4). Hoffman5 affirmed that training at or above 60–70% of maximum HR will provide a sound basis for design of an endurance exercise programme for individuals with SCI.
Such improvements in endurance are confirmed by the VT, usually expressed as a percentage of peak , which could be considered as a key parameter of the endurance capacity and often good predictor of endurance performance.28 Results in this study (61% before training and 70% after training) are in accordance with those of Flandrois et al29 (59% of peak) and Coutts et al30 (69% of peak).30
This is objectively confirmed by the very large rise in the TPW (+24.7%) between the first and the last session, whereas HR did not change. These results indicate that for the same HR, the patients were able to perform a higher TPW and increased their work capacity. As well, the same exercise session performed after training induces a lower physiological stress since VE and HR were significantly lower.
As expected, a significant increase was observed in peak (+16%) that can be considered as a valid indicator for the improvement of physical fitness and work capacity.
Hoffmann5 summarised the results of 13 cardiorespiratory training studies on wheelchair users, noting an average improvement in max of 20% (range 0–61%) after 4–20 weeks of training.
Differences between this study and their studies can be explained by the diversity of the programmes and the heterogeneousness of the subjects.
According to the age, sex, level, length and the origin of the lesion, the habitual activities, the professional situation, and training level, the values obtained are variable.
During wheelchair propulsion, muscles of arm and forearm are active. As improvements were obtained during peak loads, there were likely modifications about the change or time course of girth after the training session, which has been shown on able-bodied subjects with a similar training programme (Tordi et al26). They measured morphologic parameters such as diameter and circumference of the right upper arm and forearm. They observed significant improvements in circumference and diameter of the arm and forearm after training. In this study, as the exercise was the same, and as the lesion was not influencing the performances with the superior members, similar muscle modifications as able-bodied subjects probably occurred. Unfortunately, these measures were not taken, but it will be performed in future studies.
In addition, training probably modifies the ventilation (ie higher ventilatory efficiency after training). Indeed, it has been previously described by Silva et al31 in an aerobic training programme (arm crank ergometer) with SCI patients. They studied the effects on ventilatory muscle endurance (VME). SCI patients performed 30 min training sessions, with the training target HR corresponding to VT. They observed a ‘dramatic improvement’ on VME after training and thought that it was probably because of an effective training-induced alteration on primary and accessory functionally active respiratory muscles. In the present study, subjects trained for 45 min sessions, three times a week for 6 weeks with interval training, with a minimal training target during the base corresponding at VT (Table 4). So, as the respiratory stress was quite high in this programme compared to that of Silva et al31 the same improvements were expected to have occurred.
Conclusion
It is generally agreed that cardiorespiratory fitness for wheelchair-dependent individuals could be improved with an appropriate training programme.
This training programme induces a significant improvement in physical work capacity and endurance. Indeed, training effects were observed in maximal values, endurance capacity, while submaximal power outputs encountered during daily activities induces a smaller physiological stress. These improvements can be related to the protocol's specificities that precisely respect the guidelines observed in the literature for SCI population training.
The use of the SWEET concept for SCI population training present several interests: first, it is an efficient way to improve physical fitness and second, it is a way to obtain a more homogeneous protocol between the different rehabilitation programmes proposed to deficient populations. Differences obtained between this study and Tordi's study merit consideration if a 4- or 6-week programme is better in function of the subjects considered.
References
Janssen TWJ, Vanoers CAJM, Vanderwoude LHV, Hollander AP . Physical strain in daily life of wheelchair users with spinal-cord injuries. Med Sci Sport Exerc 1994; 26: 661–670.
Le CT, Price M . Survival from spinal cord injury. J of Chronic Dis 1982; 35: 487–492.
Linn WS, Adkins RH, Gong H, Waters RL . Pulmonary function in chronic spinal cord injury: a cross-sectional survey of 222 Southern California adult outpatients. Arch Phys Med Rehabil 2000; 81: 757–763.
Cowell LL, Squires WG, Raven PB . Benefits of aerobic exercise for the paraplegic: a brief review. Med Sci Sports Exerc 1986; 18: 501–508.
Hoffman MD . Cardiorespiratory fitness and training in quadriplegics and paraplegics. Sports Med 1986; 3: 312–330.
Glaser RM, Suryaprasad AG, Sawka MN, Fichtenbaum BM . Methodology devised for a program to improve efficiency and reduce risks for wheelchair locomotion. Bull Prosthet Res 1981; 10: 63–68.
Sawka MN, Glaser RM, Wilde SW, Von Luhrte TC . Metabolic and circulatory responses to wheelchair and arm crank exercise. J Appl Physiol 1980; 49: 784–788.
DiCarlo SE, Taylor HC . Effect of arm ergometry training on physical work capacity of individuals with spinal cord injuries. Phys Ther 1983; 63: 1104–1107.
Glaser RM, Sawka MN, Brune MF, Wilde SW . Physiological responses to maximal effort wheelchair and arm crank ergometry. J Appl Physiol 1980; 48: 1060–1064.
Sedlock DA, Knowlton RG, Fitzgerald PI . The effects of arm crank training on the physiological responses to submaximal wheelchair ergometry. Eur J Appl Physiol 1988; 57: 55–59.
Dreisinger TE . Wheelchair ergometric training in the handicapped. Med Sci Sports Exerc 1979; 11: 112–113.
Dalton RB . Effects of exercise and vitamin B12 supplementation on the depression scale scores of a wheelchair confined population [thesis] Missouri University, Columbia, 1980.
Whiting RB, Dreisinger TE, Dalton RB, Londeree BR . Improved physical fitness and work capacity in quadriplegics by wheelchair exercise. J Cardiopulmonary Rehabil 1983; 3: 251–255.
Hooker SP, Wells CL . Effects of low- and moderate-intensity training in spinal cord-injured persons. Med Sci Sports Exerc 1989; 21: 18–22.
Midha M, Schmitt JK, Sclater M . Exercise effect with the wheelchair aerobic fitness trainer on conditioning and metabolic function in disabled persons: a pilot study. Arch Phys Med Rehabil 1999; 80: 258–261.
Shepard RJ . Sports medicine and the wheelchair athlete. Sports Med 1988; 5: 226–247.
Gimenez M et al. Square-wave endurance exercise test (SWEET) for training and assessment in trained and untrained subjects. III. Effect on VO2 max and maximal ventilation. Eur J Appl Physiol 1982; 49: 379–387.
Gimenez M, Servera E, Saunier C, Lacoste J . Square-wave endurance exercise test (SWEET) for training and assessment in trained and untrained subjects, II. Blood gases and acid-base balance. Eur J Appl Physiol 1982; 49: 369–377.
Gimenez M, Servera E, Salinas W . Square-wave endurance exercise test (SWEET) for training and assessment in trained and untrained subjects. I. Description and cardiorespiratory responses. Eur J Appl Physiol 1982; 49: 359–368.
Wasserman K, Hansen J, Sue D, Whipp B (eds). Principles of Exercise Testing End Interpretation. Lea and Febiger: Philadelphia 1987.
Gimenez M et al. Implications of lower- and upper-limb training procedures in patients with chronic airway obstruction. Chest 1992; 101: 279S–288S.
Devillard X et al. Validation of a new ergometer adapted to all types of manual wheelchair. Eur J Appl Physiol 2001; 85: 479–485.
Lonsdorfer J et al. Améliorations cardio-respiratoires et métaboliques aprés un entraînement par exercices en créneaux. Sci Sports 1989; 4: 161–164.
Lampert E et al. Aptitude physique et entraînement en endurance du transplanté cardiaque; proposition d'un programme court de réentraînement. Sci Sports 1994; 9: 87–92.
Lampert E et al. Short endurance training improves lactate removal ability in patients with heart transplants. Med Sci Sports Exerc 1996; 28: 801–807.
Tordi N, Gimenez M, Predine E, Rouillon JD . Effects of an interval training programme of the upper limbs on a wheelchair ergometer in able-bodied subjects. Int J Sports Med 1998; 19: 408–414.
Tordi N et al. Interval training program on a wheel-chair ergometer for paraplegic subjects. Spinal Cord 2001; 39: 532–537.
Bhambhani Y . Physiology of wheelchair racing in athletes with spinal cord injury. Sports Med 2002; 32: 23–51.
Flandrois R et al. Aerobic performance capacity in paraplegic subjects. Eur J Appl Physiol 1986; 55: 604–609.
Coutts KD, Mckenzie DC . Ventilatory thresholds during wheelchair exercise in individuals with spinal-cord injuries. Paraplegia 1995; 33: 419–422.
Silva AC et al. Effect of aerobic training on ventilatory muscle endurance of spinal cord injured men. Spinal Cord 1998; 36: 240–245.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bougenot, MP., Tordi, N., Betik, A. et al. Effects of a wheelchair ergometer training programme on spinal cord-injured persons. Spinal Cord 41, 451–456 (2003). https://doi.org/10.1038/sj.sc.3101475
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101475
Keywords
This article is cited by
-
Hybrid high-intensity interval training using functional electrical stimulation leg cycling and arm ski ergometer for people with spinal cord injuries: a feasibility study
Pilot and Feasibility Studies (2022)
-
The effectiveness of vigorous training on cardiorespiratory fitness in persons with spinal cord injury: a systematic review and meta-analysis
Spinal Cord (2021)
-
The influence of a home-based exercise intervention on human health indices in individuals with chronic spinal cord injury (HOMEX-SCI): study protocol for a randomised controlled trial
Trials (2016)
-
A 16-week randomized controlled trial evaluating the physical activity guidelines for adults with spinal cord injury
Spinal Cord (2015)
-
Coordinating arms and legs on a hybrid rehabilitation tricycle: the metabolic benefit of asymmetrical compared to symmetrical arm movements
European Journal of Applied Physiology (2014)
