
Abstract
Glioblastoma (GBM) is fatal. The standard radiotherapy and chemotherapy (temozolomide) followed by an adjuvant phase of temozolomide provide patients with, on average, a 2.5 months benefit. New treatments that can improve sensitivity to the standard treatment are urgently needed. Herein, we review the mechanisms and utility of poly (ADP-ribose) polymerase inhibitors in combination with radiation therapy as a treatment option for GBM patients and the role of phosphatase and tensin homologue mutations as a biomarker of response.
Similar content being viewed by others

Glioblastoma
Glioblastoma (GBM) is a uniformly lethal disease that has had few therapeutic advances over the past century. The standard treatment for GBM consists of radiotherapy (RT) combined with temozolomide (TMZ) chemotherapy followed by at least six cycles of TMZ. The median survival is less than 15 months. Survival is significantly worse for patients whose tumor is unmethylated at the O 6-methylguanine-DNA methyltransferase (MGMT) promoter, because they do not respond to the TMZ component of the therapy. Approximately, 50–60 % of GBMs are MGMT unmethylated, and while it is generally accepted that these patients do not respond to the standard treatment, alternative therapies for this group of patients are lacking, creating a critical unmet need.
A number of studies have investigated the use of poly (ADP-ribose) polymerase (PARP) inhibitors to inhibit the DNA repair process. PARP inhibitors include veliparib (ABT-888; Abbvie), olaparib (AstraZeneca), talazoparib (Biomarin), and niraparib (Tesaro). Veliparib and olaparib are currently being investigated in GBM patients. The Alliance study in the US randomises GBM patients with methylated MGMT promotor to the standard RT and TMZ followed by TMZ or RT and TMZ followed by TMZ and veliparib. The VERTU study in Australia is currently recruiting primary GBM patients whose tumor is unmethylated at the MGMT promoter. Patients receive veliparib in combination with radiotherapy followed by an adjuvant course of veliparib and TMZ. In the United Kingdom, the Oparatic trial is treating recurrent GBM patients with a combination of olaparib and TMZ. This review outlines the use of PARP inhibitors and irradiation in GBM and the limited and conflicting evidences, regarding the impact of mutations in the phosphatase and tensin homologue (PTEN) gene upon this treatment.
Role of PARP in DNA repair
Poly (ADP-ribose) polymerase family member 1 (PARP1) is a nuclear enzyme involved in the recruitment of repair proteins required for base excision repair (BER) and single-strand break repair (SSBR). PARP1 binds to single-strand breaks (SSB) or SSB intermediates generated during BER [1]. Upon binding, PARP1 catalyses the formation of poly ADP-ribose (pADPr) chains onto itself and other proteins, including the DNA damage scaffold protein X-ray repair cross-complementing protein 1 (XRCC1). These pADPr chains signal and attract repair proteins [2].
There is conflicting evidence regarding whether PARP1 is required for BER/SSBR [3], merely speeds it up [4], or is not essential. Following siRNA knock down of PARP1, Godon et al. [5] found SSBR continued, whilst Strom et al. [6] found that there was no accumulation of SSB intermediates. Strom et al. [6] propose that PARP1 only binds to SSB intermediates which become uncoupled during BER.
Recent studies suggest that PARP1 also binds to double-strand breaks (DSB) and may play a role in restart of collapsed DNA replication forks and in an alternative non-homologous end-joining (NHEJ) pathway [7]. PARP1 is responsible for 85–95 % of pADPr production in humans [8]. Less is known about the role of poly (ADP-ribose) polymerase family member 2 (PARP2); however, it is suggested that PARP2 acts at later stages of BER/SSBR [1].
Use of PARP inhibitors in cancer treatment
There are a number of PARP inhibiting drugs currently being tested. Most PARP inhibitors (PARPi) are competitive inhibitors, which compete with NAD+ to bind to PARP’s active site [9]. Whilst it is generally thought that PARPi act to prevent or delay SSBR, there are conflicting views regarding the mechanism(s) by which this occurs. It has been proposed that the binding of PARPi to PARP1’s active site prevents the formation of pADPr chains required to recruit repair proteins, thus delaying BER/SSBR and leading to the accumulation of SSB [10]. Alternatively, it is suggested that PARPi prevent the release of PARP1 from SSB/SSB intermediates, thereby preventing their repair [5, 9]. The latter view is consistent with findings that to dissociate from DNA; PARP1 must attach a pADPr chain to itself [11]. It also provides an explanation for findings that PARPi result in greater radiosensitivity and delays in SSBR than PARP depletion [5].
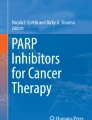
However, as noted by Lupo and Trusolino [12], these mechanisms are not mutually exclusive. Both will result in unrepaired DNA damage, which in replicating cells will lead to further damage requiring homologous recombination (HR) for repair. This could be due to persisting SSB causing collapse of replication forks and the generation of DSB during DNA replication [13, 14]. Alternatively, further damage could be due to trapped PARP-DNA complexes preventing DNA replication and requiring HR for repair [9]. Figure 1 illustrates the role of PARP1 in SSB DNA repair and the mechanisms by which PARPi are thought to generate further damage. The investigations of PARPi in cancer treatment have focused upon their use to potentiate the effects of chemotherapy and/or radiotherapy and their use as a single agent in tumors with defects in HR [15].

Poly (ADP-ribose) polymerase family member 1 (PARP1) and PARP inhibitors (PARPi) in single-strand break DNA repair. a Simplified diagram showing the function of PARP1 in single-strand break DNA repair. PARP1 binds to single-strand breaks (SSB)/SSB intermediates and catalyses poly ADP-ribose (pADPr) chains to recruit repair proteins, before dissociating from repaired DNA. b Illustrates the effect of PARPi on PARP1. After binding to SSB/SSB intermediates, PARP1 is unable to catalyse a pADPr chain to recruit repair proteins. It has been suggested in the absence of repair proteins, PARP will dissociate from the DNA, leaving an unrepaired single-strand break which will cause collapse of the replication fork during DNA replication, generating a double-strand break that requires homologous recombination (HR) for repair. Alternatively, it is proposed that PARP1’s inability to catalyse a pADPr chain will result in PARP1 remaining bound to the single-strand break, hindering DNA replication, and requiring HR for repair
Use of PARPi to potentiate irradiation
The primary mechanism by which ionising radiation causes damage is through the generation of free radicals that interact with DNA [16]. Whilst these interactions can damage nucleotides and lead to SSB and DSB, SSB are the most prevalent [15]. Damage to nucleotides and SSB is primarily repaired by BER/SSBR, whilst DSB are repaired primarily by NHEJ [13]. However, DSB which occur during DNA replication are repaired by HR [17].
The use of PARPi, to inhibit or delay the BER/SSBR process, in combination with irradiation can, therefore, assist in converting radiation-induced nucleotide damage and SSB into more toxic DSB [15]. However, as demonstrated by Noel et al. [18], this will only occur in replicating cells.
Whilst cells proficient in double-strand break repair (DSBR) can fix this damage, given the amount of damage irradiation can induce in a short period, it is possible that these repair mechanisms may become overwhelmed [19]. Based upon studies implicating PARP1 in the recruitment of proteins involved in replication fork restart, it is possible that PARPi may directly effect this HR-mediated process [7]. PARPi and irradiation could also take advantage of defects in DSBR pathways [20], such as reduced expression of HR proteins which has been found in hypoxic cells [21]. In the absence of repair, DSB can result in cell-cycle arrest, apoptosis, or senescence [17].
The use of PARPi in combination with irradiation has been shown to increase the radiosensitivity of commercial GBM cell lines [13, 14, 22], primary GBM initiating cells [23], and in in vivo studies [14]. However, the findings of Venere et al. [23] suggest that the radiosensitising effects may be primarily due to their impact upon GBM initiating cells (GIC), with decreased viability only seen in one of the three non-GIC specimens. There is, however, criticism of the marker used by Venere et al. [23] to identify GIC’s, with studies showing that CD133+ cells are not the only cells with initiating properties [24]. Furthermore, as the cell lines used in the other studies would also have contained GIC’s, these results are not necessarily contradictory.
In contrast to these studies, Clarke et al. [25] found veliparib and irradiation resulted in no additional survival benefit compared with irradiation alone, using the primary GBM orthotopic models. Surprisingly, they also found veliparib and TMZ had a greater effect than combined veliparib, TMZ, and irradiation in the GBM12 cell line, whilst the results in the GBM22 cell line were not significant. However, as acknowledged by the authors, these results are based upon very limited data. Majuelos-Melguizo et al. [26] reported no additional benefit from the use of veliparib and irradiation compared with veliparib alone in commercial GBM cell lines. However, they do not include any data to support these findings and unlike the other in vitro studies, appear to rely upon an MTT assay to measure cell viability, rather than clonogenic survival assays. Given the limitations of these studies, the weight of evidence tends to suggest that PARPi radiosensitise GBM.
PARPi and synthetic lethality
The use of PARPi alone in breast cancer 1 and/or breast cancer 2 (together BRCA) deficient cells has been shown to result in increased sensitivity. The BRCA proteins play an essential role in HR and it is believed that PARPi-induced effects upon SSBR, in cells deficient in HR, result in synthetic lethality [27]. As GBM’s do not commonly have defects in genes coding for proteins directly involved in HR [16], it is not known what factors may mediate sensitivity to PARPi in these tumors.
PTEN
PTEN is located on the long arm of chromosome 10 and codes for a lipid and protein phosphatase. PTEN contains a phosphatase domain in its N terminal region and a C terminal region believed to play a role in the nucleus [28]. Loss of one allele of the long arm of chromosome 10 is found in 70 % of GBM patients, with somatic mutations occurring in 25–40 % of cases [29].
PTEN’s role in the PI3 K/Akt pathway
In the cytoplasm, PTEN negatively regulates the phosphoinositide 3-kinase (PI3 K)/Akt pathway, through its dephosphorylation of phosphatidylinositol 3,4,5-trisphosphate (PIP3). The pathway is activated by the binding of growth factors to tyrosine kinase receptors, which, in turn, activate PI3 K, which phosphorylates phosphatidylinositol 4,5-bisphosphate (PIP2) to generate PIP3 [29]. In the absence of PTEN, PIP3 phosphorylates Akt, which, in turn, phosphorylates other molecules involved in cell-cycle progression, growth, angiogenesis, and the inhibition of apoptosis [30].
The loss of PTEN has been linked to radioresistance, as a result of unchecked activation of Akt and Akt’s negative effect upon levels of checkpoint kinase 1 (Chk1). Chk1 plays a critical role in suppressing DNA replication and activating G2/M cell-cycle arrest to allow time for DNA repair [31].
Studies have shown PTEN mutations confer radioresistance in GBM. Wick et al. [32] and Kao et al. [33] demonstrated the introduction of the PTEN gene to PTEN mutant (PTEN mt) GBM cell lines sensitised the cells to irradiation. The former study demonstrated that the phosphatase domain of PTEN was required for this effect. Kao et al. [33] also showed the introduction of PTEN decreased levels of phosphorylated Akt and led to the persistence of γ-H2AX, a marker for unrepaired DSB. McEllin et al. [34] reported that GBM cell lines deficient in PTEN were more radioresistant and found that the deletion of PTEN in murine astrocytes resulted in radioresistance. The addition of PTEN has also been shown to lead to radiosensitivity and impaired DSBR in PTEN mt lung and prostate cancer cells [35, 36]. However, Fraser et al. [37] found that the depletion of PTEN in primary prostate cancer cells led to radiosensitivity, leading the authors to suggest cells which develop in the absence of PTEN which may function differently to those, in which PTEN is experimentally removed.
PTEN’s role in the nucleus
Significantly less is known about PTEN’s role in the nucleus. In addition to contributing to chromosomal integrity, it has been suggested that PTEN regulates RAD51 [38]. RAD51 is recruited to the site of collapsed replication forks and plays an essential role in HR [13]. Although subsequent studies have moved away from the notion that PTEN directly regulates RAD51, many studies suggest PTEN mutations affect DSBR. There is, however, a little consensus regarding the mechanism(s) by which this occurs. Mendes-Pereira et al. [39] reported a reduction in RAD51 foci following DNA damage, whilst McEllin et al. [34] found a decrease in RAD51 paralogs, believed to assist RAD51, in PTEN mt astrocytes. Using embryonic kidney cells, Mukherjee and Karmakar [40] found reduced RAD51 foci and loss of the G2/M checkpoint in PTEN mt cells. Minami et al. [41] reported reduced RAD51 foci and levels of MRE11, which is also involved in HR, in PTEN mt lung cancer cells. More recently, He et al. [42] (2015) found RAD51 dissociated from replication forks in PTEN null HeLa cells, suggesting that PTEN may play a role in recruiting RAD51 to collapsed replication forks.
However, there are also studies suggesting that PTEN mutations may have no effect upon HR. Using the same cell lines as Shen et al. [38], Gupta et al. [43] found no reduction in RAD51, nor increased residual DNA damage in PTEN mt cells. Differences in the findings have been attributed to different methods used [44], with the findings of Shen et al. [38] based on spontaneously arising DSB, whilst Gupta et al. [43] used irradiation prior to measuring DSB. The studies also used different antibodies to detect RAD51, which Gupta et al. [38] found led to markedly different results. Fraser et al. [37] also reported finding no association between PTEN status, RAD51, and HR in primary prostate cancer cells. Despite this, they found the use of siRNA to knock down PTEN in H1299 lung cancer cells resulted in increased sensitisation to PARPi. In light of their conflicting findings, they suggest that there may be a difference in the phenotype of cells that develop without PTEN and those in which PTEN is knocked down using siRNA. However, this does not explain contrary findings in cell lines, where the PTEN expression was not experimentally reduced [39, 41]. Fraser et al. [37] also propose that the interaction between PTEN and DSBR pathways may be cell/tissue specific. The findings of Miyasaka et al. [45] suggest that this could be the case, with PTEN mt cells in endometrial cancer cell lines showing both the greatest and least levels of resistance to PARPi.
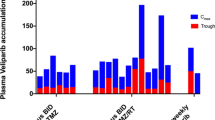
The potential interaction between PTEN and RAD51 has led to studies investigating the use of PARPi in PTEN mt cells. Mendes-Pereira et al. [39] used PARPi in a range of commercial tumor cell lines, including GBM, finding a significant reduction in HR in PTEN mt cells. However, only cells with mutations in the C terminal of PTEN (PTENC−) displayed increased sensitivity to PARPi, whilst those with mutations limited to the N terminal (PTENN−) were resistant. Consistent with these findings, Gong et al. [46] found that PTEN wt cells were less sensitive to PARPi, whilst PTENC− cells showed similar sensitivity to PTEN null cells. Sun et al. [47] reported increased DSB in PTEN null and PTEN C− cells. These findings suggest that it is the loss of the PTEN C terminal that confers sensitivity to PARPi and may provide an explanation for the different findings regarding PARPi and PTEN status. The broadly agreed the role of the two regions of PTEN and the potential effect of mutations in these regions is summarised in Fig. 2.

Location of the PTEN mutation may determine the response to PARP inhibitors (PARPi) and irradiation. Summary of the proposed effects of irradiation and PARPi upon the N and C terminal regions of PTEN, the impact of mutations in each region, and the mechanisms by which these effects are thought to occur. The status of the phosphatase domain in the N terminal region of PTEN has an impact upon the cells response to irradiation. Cells with functional N terminal regions are radiosensitive, whilst those with mutations in this region are more radioresistant. Mutations in the C terminal region may impact upon the cells response to PARPi. Cells with mutations in the C terminal region of PTEN have been shown to be sensitive to PARPi, whilst those with functional C terminal regions have been shown to be resistant to PARPi. PBD PIP2-binding domain, DSBR double-strand break repair
Use of PARPi and irradiation in PTEN mt GBM
Examination of earlier studies that included GBM cell lines with known PTEN mutations provides conflicting evidence. Dungey et al. [13] found that the use of PARPi did not increase radiosensitivity or reduce cell survival in U87MG PTEN mt GBM cells, whilst Barazzuol et al. [22] found a modest radiosensitising effect in this cell line. Conversely, U251MG PTEN mt GBM cells were highly sensitised to PARPi and irradiation [13, 14, 22]. Whether these differences are potentially attributable to the TP53 mt present in U251MG cells [48], the location of the PTEN mutation is the evidence that different cells may respond differently to PARPi is unknown.
Summary
Approximately 70 % of GBM patients harbor mutations in the PTEN gene. It is, therefore, imperative that we gain a better understanding of the role of PTEN in mediating the response to treatment with PARPi and irradiation. However, evidence in the literature regarding the role of PTEN and the response to PARPi in GBM is limited and conflicting. It is estimated that >50 genes, many mutated in cancer, can confer sensitivity to PARPi. It is, therefore, important that we test all patient tumors that are enrolled in PARPi clinical trials for biomarkers of clinical response.
References
De Vos M, Schreiber V, Dantzer F. The diverse roles and clinical relevance of PARPs in DNA damage repair: current state of the art. Biochem Pharmacol. 2012;84(2):137–46.
Gibson BA, Kraus WL. New insights into the molecular and cellular functions of poly(ADP-ribose) and PARPs. Nat Rev Mol Cell Biol. 2012;13(7):411–24.
El-Khamisy SF, Masutani M, Suzuki H, Caldecott KW. A requirement for PARP-1 for the assembly or stability of XRCC1 nuclear foci at sites of oxidative DNA damage. Nucleic Acids Res. 2003;31(19):5526–33.
Mortusewicz O, Amé J-C, Schreiber V, Leonhardt H. Feedback-regulated poly(ADP-ribosyl)ation by PARP-1 is required for rapid response to DNA damage in living cells. Nucleic Acids Res. 2007;35(22):7665–75.
Godon C, Cordelières FP, Biard D, Giocanti N, Mégnin-Chanet F, Hall J, et al. PARP inhibition versus PARP-1 silencing: different outcomes in terms of single-strand break repair and radiation susceptibility. Nucleic Acids Res. 2008;36(13):4454–64.
Ström CE, Johansson F, Uhlén M, Szigyarto CA-K, Erixon K, Helleday T. Poly (ADP-ribose) polymerase (PARP) is not involved in base excision repair but PARP inhibition traps a single-strand intermediate. Nucleic Acids Res. 2011;39(8):3166–75.
Beck C, Robert I, Reina-San-Martin B, Schreiber V, Dantzer F. Poly (ADP-ribose) polymerases in double-strand break repair: focus on PARP1, PARP2 and PARP3. Exp Cell Res. 2014;329(1):18–25.
Balvers RK, Lamfers ML, Kloezeman JJ, Kleijn A, Pont LMB, Dirven CM, et al. ABT-888 enhances cytotoxic effects of temozolomide independent of MGMT status in serum free cultured glioma cells. J Transl Med. 2015;13(1):74–83.
Murai J, Shar-yin NH, Das BB, Renaud A, Zhang Y, Doroshow JH, et al. Trapping of PARP1 and PARP2 by clinical PARP inhibitors. Cancer Res. 2012;72(21):5588–99.
Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature. 2005;434(7035):913–7.
Donawho CK, Luo Y, Luo Y, Penning TD, Bauch JL, Bouska JJ, et al. ABT-888, an orally active poly(ADP-ribose) polymerase inhibitor that potentiates DNA-damaging agents in preclinical tumor models. Clin Cancer Res. 2007;13(9):2728–37.
Lupo B, Trusolino L. Inhibition of poly(ADP-ribosyl)ation in cancer: old and new paradigms revisited. Biochim Biophys Acta (BBA) Rev Cancer. 2014;1846(1):201–15.
Dungey FA, Löser DA, Chalmers AJ. Replication-dependent radiosensitization of human glioma cells by inhibition of poly(ADP-ribose) polymerase: mechanisms and therapeutic potential. Int J Radiat Oncol Biol Phys. 2008;72(4):1188–97.
Russo AL, Kwon H-C, Burgan WE, Carter D, Beam K, Weizheng X, et al. In vitro and In vivo Radiosensitization of Glioblastoma Cells by the Poly (ADP-Ribose) Polymerase Inhibitor E7016. Clin Cancer Res. 2009;15(2):607–12.
Curtin NJ, Szabo C. Therapeutic applications of PARP inhibitors: anticancer therapy and beyond. Mol Asp Med. 2013;34(6):1217–56.
Alexander BM, Ligon KL, Wen PY. Enhancing radiation therapy for patients with glioblastoma. Expert Rev Anticancer Ther. 2013;13(5):569–81.
Helleday T, Petermann E, Lundin C, Hodgson B, Sharma RA. DNA repair pathways as targets for cancer therapy. Nat Rev Cancer. 2008;8(3):193–204.
Noël G, Godon C, Fernet M, Giocanti N, Mégnin-Chanet F, Favaudon V. Radiosensitization by the poly(ADP-ribose) polymerase inhibitor 4-amino-1,8-naphthalimide is specific of the S phase of the cell cycle and involves arrest of DNA synthesis. Mol Cancer Ther. 2006;5(3):564–74.
Dungey FA, Caldecott KW, Chalmers AJ. Enhanced radiosensitisation of human glioma cells by combining inhibition of PARP with inhibition of Hsp90. Mol Cancer Ther. 2009;8(8):2243–54.
Löser DA, Shibata A, Shibata AK, Woodbine LJ, Jeggo PA, Chalmers AJ. Sensitization to radiation and alkylating agents by inhibitors of poly(ADP-ribose) polymerase is enhanced in cells deficient in DNA double-strand break repair. Mol Cancer Ther. 2010;9(6):1775–87.
Chan N, Koritzinsky M, Zhao H, Bindra R, Glazer PM, Powell S, et al. Chronic hypoxia decreases synthesis of homologous recombination proteins to offset chemoresistance and radioresistance. Cancer Res. 2008;68(2):605–14.
Barazzuol L, Jena R, Burnet NG, Meira LB, Jeynes JCG, Kirkby KJ, et al. Evaluation of poly (ADP-ribose) polymerase inhibitor ABT-888 combined with radiotherapy and temozolomide in glioblastoma. Radiat Oncol (Lond Engl). 2013;8:65–75.
Venere M, Hamerlik P, Wu Q, Rasmussen R, Song L, Vasanji A, et al. Therapeutic targeting of constitutive PARP activation compromises stem cell phenotype and survival of glioblastoma-initiating cells. Cell Death Differ. 2014;21(2):258–69.
Brescia P, Richichi C, Pelicci G. Current strategies for identification of glioma stem cells: adequate or unsatisfactory? J Oncol. 2012;2012:10.
Clarke MJ, Mulligan EA, Grogan PT, Mladek AC, Carlson BL, Schroeder MA, et al. Effective sensitization of temozolomide by ABT-888 is lost with development of temozolomide resistance in glioblastoma xenograft lines. Mol Cancer Ther. 2009;8(2):407–14.
Majuelos-Melguizo J, Rodríguez MI, López-Jiménez L, Rodríguez-Vargas JM, Martí Martín-Consuegra JM, Serrano-Sáenz S, et al. PARP targeting counteracts gliomagenesis through induction of mitotic catastrophe and aggravation of deficiency in homologous recombination in PTEN-mutant glioma. Oncotarget. 2015;6(7):4790–803.
Javle M, Curtin NJ. The role of PARP in DNA repair and its therapeutic exploitation. Br J Cancer. 2011;105(8):1114–22.
Yin Y, Shen WH. PTEN: a new guardian of the genome. Oncogene. 2008;27(41):5443–53.
Chalhoub N, Baker SJ. PTEN and the PI3-Kinase pathway in cancer. Annu Rev Pathol. 2009;4:127–50.
Baker SJ, McKinnon PJ. Tumour-suppressor function in the nervous system. Nat Rev Cancer. 2004;4(3):184–96.
Hunt CR, Gupta A, Horikoshi N, Pandita TK. Does PTEN loss impair DNA double-strand break repair by homologous recombination? Clin Cancer Res. 2012;18(4):920–2.
Wick W, Furnari FB, Naumann U, Cavenee WK, Weller M. PTEN gene transfer in human malignant glioma: sensitization to irradiation and CD95L-induced apoptosis. Oncogene. 1999;18(27):3936–43.
Kao GD, Jiang Z, Fernandes AM, Gupta AK, Maity A. Inhibition of phosphatidylinositol-3-OH kinase/Akt signaling impairs DNA repair in glioblastoma cells following ionizing radiation. J Biol Chem. 2007;2007:21206–12.
McEllin B, Camacho CV, Mukherjee B, Hahm B, Tomimatsu N, Bachoo RM, et al. PTEN loss compromises homologous recombination repair in astrocytes: implications for GBM therapy with temozolomide or PARP inhibitors. Cancer Res. 2010;70(13):5457–64.
Pappas G, Zumstein LA, Munshi A, Hobbs M, Meyn RE. Adenoviral-mediated PTEN expression radiosensitizes non-small cell lung cancer cells by suppressing DNA repair capacity. Cancer Gene Ther. 2007;14(6):543–9.
Rosser CJ, Tanaka M, Pisters LL, Tanaka N, Levy LB, Hoover DC, et al. Adenoviral-mediated PTEN transgene expression sensitizes Bcl-2-expressing prostate cancer cells to radiation. Cancer Gene Ther. 2004;11(4):273–9.
Fraser M, Zhao H, Luoto KR, Lundin C, Coackley C, Chan N, et al. PTEN deletion in prostate cancer cells does not associate with loss of RAD51 function: implications for radiotherapy and chemotherapy. Clin Cancer Res. 2012;18(4):1015–27.
Shen WH, Balajee AS, Wang J, Wu H, Eng C, Pandolfi PP, et al. Essential role for nuclear PTEN in maintaining chromosomal integrity. Cell. 2007;2007:157–70.
Mendes-Pereira AM, Martin SA, Brough R, McCarthy A, Taylor JR, Kim JS, et al. Synthetic lethal targeting of PTEN mutant cells with PARP inhibitors. EMBO Mol Med. 2009;1(6–7):315–22.
Mukherjee A, Karmakar P. Attenuation of PTEN perturbs genomic stability via activation of Akt and down-regulation of Rad51 in human embryonic kidney cells. Mol Carcinog. 2013;52(8):611–8.
Minami D, Takigawa N, Takeda H, Takata M, Ochi N, Ichihara E, et al. Synergistic effect of olaparib with combination of cisplatin on PTEN-deficient lung cancer cells. Mol Cancer Res. 2013;11(2):140–8.
He J, Kang X, Yin Y, Chao KSC, Shen WH. PTEN regulates DNA replication progression and stalled fork recovery. Nat Commun. 2015;2015:6.
Gupta A, Yang Q, Pandita RK, Hunt CR, Xiang T, Misri S, et al. Cell cycle checkpoint defects contribute to genomic instability in PTEN deficient cells independent of DNA DSB repair. Cell Cycle. 2009;8(14):2198–210.
Ming M, He Y-Y. PTEN in DNA damage repair. Cancer Lett. 2012;319(2):125–9.
Miyasaka A, Oda K, Ikeda Y, Wada-Hiraike O, Kashiyama T, Enomoto A, et al. Anti-tumor activity of olaparib, a poly (ADP-ribose) polymerase (PARP) inhibitor, in cultured endometrial carcinoma cells. BMC Cancer. 2014;14(1):1–10.
Gong L, Govan JM, Evans EB, Dai H, Wang E, Lee S-W, et al. Nuclear PTEN tumor-suppressor functions through maintaining heterochromatin structure. Cell Cycle. 2015;14(14):2323–32.
Sun Z, Huang C, He J, Lamb Kristy L, Kang X, Gu T, et al. PTEN C-terminal deletion causes genomic instability and tumor development. Cell Reports. 2014;6(5):844–54.
Godoy PRDV, Mello SS, Magalhães DAR, Donaires FS, Nicolucci P, Donadi EA, et al. Ionizing radiation-induced gene expression changes in TP53 proficient and deficient glioblastoma cell lines. Mutat Res, Genet Toxicol Environ Mutagen. 2013;756(1–2):46–55.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Lester, A., Rapkins, R., Nixdorf, S. et al. Combining PARP inhibitors with radiation therapy for the treatment of glioblastoma: Is PTEN predictive of response?. Clin Transl Oncol 19, 273–278 (2017). https://doi.org/10.1007/s12094-016-1547-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-016-1547-4