
Abstract
Summary
Critical illness may lead to altered bone turnover and associated adverse health outcomes. This systematic review found moderate evidence for a positive association between critical illness and increased bone turnover. Prospective cohort studies that identify the extent and risk factors for critical illness related bone loss are required.
Introduction
Intensive care patients face health issues that extend beyond their critical illness and result in significant morbidity and mortality. Critical illness may result in altered bone turnover due to associated immobilisation, inflammation, exposure to medications that effect bone and calcium metabolism, and endocrine dysfunction. The aim of this study was to synthesise the existing evidence for altered bone turnover in adults admitted to intensive care.
Methods
A literature search using MEDLINE and EMBASE was performed from 1965 to March 2013. Reviewed studies investigated the relationship between critical illness and evidence of altered bone turnover (bone turnover markers, bone mineral density, or fracture). Studies were rated upon their methodological quality, and a best-evidence synthesis was used to summarise the results.
Results
Four cohort and seven case–control studies were identified for inclusion, of which five studies were rated as being of higher methodological quality. Ten of the studies measured bone turnover markers, and one study fracture rate. Findings were consistent across studies, and best-evidence analysis resulted in a conclusion that moderate evidence exists for an association between critical illness requiring admission to intensive care and altered bone turnover.
Conclusion
A positive association between critical illness requiring intensive care admission and bone turnover exists, although data are limited, and the risk factors and the nature of the relationship are not yet understood. Prospective cohort studies that identify risk factors and extent of critical illness related bone turnover changes are required.
Similar content being viewed by others


Introduction
Intensive care patients face health issues after their critical illness including increased mortality, reduced quality of life, reduced return to work, and ongoing economic and social costs to families and caregivers when compared to pre-illness and general population controls [1–7]. Despite an increasing awareness of long-term sequelae of critical illness, the identification of specific pathophysiologies amenable to intervention remains elusive. Osteoporosis is a major public health problem, and is widely recognised as a chronic progressive disease with multifactorial aetiology [8]. The epidemiology and risk factors for primary and secondary osteoporosis are well described, including increasing age, female gender, low body mass index (BMI), smoking, excessive alcohol intake, positive family history, medications such as glucocorticoids, and predisposing disease or medical condition such as hyperthyroidism [8, 9]. However, as few as 13–27 % of patients with osteoporosis are treated following a fragility fracture, suggesting it remains an under-diagnosed disease [10, 11]. Critical illness, with its associated immobilisation, inflammation, and endocrine dysfunction, may lead to accelerated bone turnover. When combined with an ageing population with undiagnosed osteoporosis, this accelerated bone turnover may contribute to the burden of morbidity and mortality observed in survivors of intensive care [12, 13]. In a review of metabolic bone disease in the intensive care unit (ICU), Hollander et al. concluded an interventional study of bisphosphonates in survivors of ICU is needed [14]. However, there is no systematic review of the evidence for accelerated bone turnover following critical illness, or of the nature and risk factors for this relationship.
In this study, we sought to systematically review and synthesise the current literature regarding the association between critical illness and changes to bone turnover. In addition, we describe ongoing and planned research in this area.
Methods
Search strategy and study selection
To identify studies that examined whether admission to an ICU was associated with changes in bone turnover in adults, we searched MEDLINE (1965 until 31 March 2013) and EMBASE (1974 until 31 March 2013) for citations of relevant articles. Our computerised search strategy employed the following medical subject headings (MeSH/EMTREE) (“mechanical ventilation” or “critical illness” or “chronic critical illness” or “ventilator” or “critical care” or “intensive care”) and (“bone turnover” or “bone change” or “fracture” or “bone mineral density” or “bone density” or “bone loss” or “CTX” or “P1NP” or “bone biomarkers” or “bone markers”).
Studies were deemed eligible for inclusion in this review if they met the following criteria: full-text original articles; comprised either a cohort, case–control, or a cross-sectional study design; examined, in adults aged ≥18 years, associations between receiving mechanical ventilation in an ICU (with a length of stay 24 h or greater), and de novo change in bone turnover (defined as loss of BMD, increase in bone turnover markers (BTMs), or incident fracture of at least one of the major osteoporotic sites of hip, wrist, humerus, or spine). Patients that were identified as osteoporotic at the time of ICU admission were included.
Studies were excluded if published in languages other than English; utilised animal models; investigated patients with existing neurological illness that results in impaired weight-bearing (including stroke with loss of weight-bearing, spinal cord injury, progressive neurological disease, e.g. multiple sclerosis); were admitted to ICU for reasons of trauma-related fracture, or with existing metabolic bone disease; employed qualitative methodology; or were review articles, editorials, commentaries, dissertations, or were randomised control trials. Where interventional studies reported baseline data that fulfilled inclusion and exclusion criteria prior to intervention, the baseline data were included in the analysis.
We electronically restricted our search to identify articles that were related to human subjects, published in English, and available in full-text. Reference lists of relevant studies deemed eligible for inclusion were manually searched, and citations were tracked for those publishing in the field of interest.
Two reviewers confirmed the search strategy (NRO and SLB) and one reviewer performed the computerised search and initial manual search (NRO). Complete details of the search strategy can be obtained from the corresponding author. For each eligible study, two reviewers (NRO and CEC) confirmed the selection of articles based on readings of the full-text article. Where the eligibility of studies was ambiguous, two reviewers (NRO and CEC) held discussions to reach consensus. Where consensus could not be achieved, a third reviewer was consulted (SLB).
Methodological quality assessment
To assess the methodological quality (internal validity) of the included studies, two reviewers (NRO and CEC) undertook independent scoring using an adapted version of the scoring system published by Lievense et al. [15] (Table 1); this methodological approach has previously been employed for reviews of observational studies in the field of musculoskeletal disorders [15, 16]. Both reviewers independently scored each of the criteria as positive (1), negative (0), or not applicable (NA), with a maximum possible score for each study design of 100 %. Where the score afforded to certain criteria differed between the reviewers, discussion was held to achieve consensus; if disagreements were not resolved, a third reviewer (SLB) was consulted to achieve a final judgment. Positive scores were summed to give an overall internal validity score.
Data analysis
As there were limited data and studies were heterogeneous, a “best-evidence” synthesis was preferred rather than a meta-analysis. The studies were divided into subgroups according to the type of study design. A cohort study was judged the most valid design, followed by case–control study. Studies were then ranked according to their methodological quality score (Table 2). A study was considered to be of higher quality if the methodological quality score was greater than the mean quality score of all studies [15–17].
Results
Search results and study characteristics
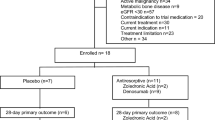
The results of our search are presented in Fig. 1. Our electronic search strategy identified 13,185 studies, including 2,218 duplicates that were subsequently excluded. Of the remaining 10,967 studies, a total of 21 underwent full-text review to determine eligibility. A further six studies were identified for full-text review from a manual search of citation lists. Of the 27 full-text studies reviewed, 16 were excluded for not meeting the predetermined eligibility criteria, resulting in 11 studies included in the final analysis [18–28]. In three of the case–control studies, ICU patients were randomised to an intervention after comparison of baseline data from the ICU cohort was compared to a control cohort [22, 23, 26]. The baseline data from these studies was included in the analysis, whereas the data resulting from the randomised intervention was excluded. One study performed in vivo analysis of osteoclast number and activity in ICU patients compared to controls, with further in vitro analysis of osteoclast cells, osteoblastic cells, and serum activation factors [25]. As the in vitro tests were not recognised tests of bone turnover, they were excluded from the analysis.

Summary of systematic search (QUOROM diagram)
Description of the studies
An overview of the included articles (n = 11) is presented in Table 3. Four of the studies were cohort study design [18–21] and the remaining seven were case–control study design [22–28]. Sample sizes ranged from 9 [28] to 739 cases [18]. A group of seven patients were shared by two studies, in which a total of 15 cases [23] and 33 cases [22] were enrolled. In addition, these studies shared the same group of 50 controls.
The criteria for enrolment in the studies included requirement for mechanical ventilation in an ICU [20, 27, 28], duration of mechanical ventilation greater than 48 h [18] or 2 weeks [22–24], chronic critical illness [25], admission to a respiratory care unit for prolonged ventilatory support [19, 21], and ICU length of stay greater than 10 days [26]. Patient populations included mixed adults in nine of the studies [18–21, 24–28], and males only in two studies [22, 23]. A control population was present in the seven case–control studies, and in one of the cohort studies [18]. The controls were age- and gender-matched healthy population-based participants in six studies [18, 22–26], age but not gender-matched healthy controls in one study [28], and non-gender or age-matched participants with a history of rheumatism or mild osteoarthritis in one study [27]. Exclusion criteria included renal, metabolic, and liver disease in five studies [22–24, 26, 28], metabolic and neurological disease in four studies [22–24], and prior medications in four studies [22–24, 26]. The follow-up time for patients ranged from 1 day [24, 25] to 10 years [18].
Methodological quality assessment
The two reviewers scored 129 items and agreed on 117 items (90.70 % agreement, κ = 0.80, standard error (SE) 0.05, 95 % CI 0.70–0.91, strength of agreement considered “very good”). The 12 disagreements were resolved in a single consensus meeting. The range of methodological scores was 55 to 67 % (Table 4), with the mean of quality scores 61 %. Using the mean score as the cut-off point, 5 of 11 were considered to be of higher methodological quality [18, 19, 22–24].
Results of all included studies
Assessment of bone turnover
Table 4 presents the findings of the reviewed studies. The BTM used in the studies included bone resorption and bone formation markers [29]. The bone resorption markers measured included urinary collagen type 1 cross-linked N-telopeptide (NTX) in two studies [19, 21], urinary pyridinoline (Pyd) or deoxypyridinoline (Dpd) in seven studies [20, 22, 23, 26–28], and urine or serum carboxy-terminal cross-linked telopeptide of type 1 collagen (ICTP/BCTX) in two studies [20, 26]. One study reported serum osteoclast precursors (double-positive CD14+/CD11b+) and serum mature osteoclasts (triple-positive CD14+/CD11b+/VNR+) [25]. Bone formation markers were reported in four studies [22–24, 26] and included serum skeletal alkaline phosphatase (SALP), serum osteocalcin (OC), serum procollagen type 1 C peptide (P1CP), and serum procollagen type 1 N peptide (P1NP). Incident fracture rate post-ICU discharge was reported as the outcome in one study [18].
Results of bone turnover measurement
All studies that measured markers of bone resorption reported an increase in markers compared to controls or reference range, suggesting increased osteoclastic activity. The two studies observing urinary NTX levels in patients admitted to a respiratory care unit (prolonged ventilation unit) reported elevated NTX in 83 % of patients [21], with baseline levels 4- to 6-fold greater than reference range [19, 21] while urinary collagen cross links (Pyd, Dpd) were increased 4- to 14-fold compared to controls [20, 22–24, 26–28], and serum carboxy-terminal cross-linked telopeptide of type 1 collagen was increased 3- to 6-fold compared to controls or reference values [20, 26]. The one study that measured osteoclast precursors and mature osteoclasts in serum described a significant increase in osteoclast precursors in critical illness compared to controls [25].
The studies that reported markers of bone formation described a varied increase in SALP compared to controls, a significant increase in P1CP and P1NP compared to controls, and a significant decrease in osteocalcin compared to controls [22–24, 26]. These results suggest an increase in number and activity of immature osteoblasts, with low activity of mature osteoblasts.
The single study that reported the incidence of new fractures following ICU described an increased incident fragility fracture risk in older female ICU survivors (rate 4.33/100 patient years, 95 % CI 2.72–5.93) compared with age- and gender-matched population controls (rate 2.81/100 patient years, 95 % CI 2.33–3.28) [18].
Exposure variables and increased bone turnover
Three studies reported a relationship between bone resorptive markers and either ICU or hospital length of stay, with a positive correlation between urinary NTX and ICU length of stay (r = 0.42, p < 0.01) [19], urinary NTX and both hospital (r = 0.49, p < 0.01) and ICU length of stay (r = 0.42, p < 0.01) [21], and increased urinary Pyd and Dpd in patients with an ICU length of stay of 5 days or greater compared to less than 5 days [28]. The relationship observed between vitamin D, parathyroid hormone, or calcium status was variable [19, 20]. An association between bone formation markers and inflammatory markers was observed in three studies [22–24], an inverse correlation between bone resorptive markers and thyroid hormones in one study [24], and no correlation between nitric oxide breakdown products and bone resorption markers in one study [27]. The two studies that compared ICU patients with sepsis to other ICU cohort reported an increase in bone resorption markers in sepsis compared to trauma [27] and surgery [20].
Best-evidence analysis
As the reviewed studies employed different methodology had recruited diverse populations (for example, differences in ages, gender and population sizes, among other factors), and examined varying follow-up times, we performed a best-evidence analysis to cater for the high-level heterogeneity. Our best-evidence synthesis included studies that scored above the mean (>61 %) for their methodological quality. Of the eligible studies, two cohort [18, 19] and three case–control studies [22–24] were considered to be of higher methodological quality.
The higher-quality cohort studies described an increase in bone resorption markers, with a positive correlation between markers and duration of ICU stay [19], and an increase in fragility fracture in older women following ICU admission compared to age- and gender-matched healthy controls [18]. The higher-quality case–control studies described an increase in bone resorption, a pattern of increased bone formation consistent with an increased number and activity of immature osteoblasts and decreased activity of mature osteoblasts, and a correlation between inflammatory cytokines and bone resorptive activity [22–24]. These results are consistent with findings of the lower-quality studies.
In summary, the result of our best-evidence analysis is 5 of 11 studies (two cohorts and three case–control) that were considered of higher methodological quality, with consistent results. This is consistent with a conclusion that moderate evidence exists for an association between critical illness requiring intensive care admission and changes in bone turnover.
Discussion
Overall, we identified limited but consistent data that examine the relationship between critical illness requiring ICU admission and bone turnover. A best-evidence analysis of available literature provides moderate evidence for a positive association between critical illness requiring ICU admission and increased bone turnover, a finding in all the studies identified by this analysis. There are insufficient high-quality data available about the factors contributing to the relationship between ICU admission and bone turnover to allow interpretation of the nature of this association.
This review included studies with patients admitted to ICU for mechanical ventilatory support for greater than 24 h, and assessed measures of bone turnover following ICU admission. We chose a relatively inclusive definition of critical illness for this review; as although chronic or prolonged critically ill are more likely to be at risk of increased bone turnover, the definition for chronic critical illness remains ambiguous [30], and the relationship between critical illness and bone metabolism is relatively unexplored.
The criteria for new bone turnover used in this review included BMD assessment, BTMs, and incident fracture. Measurement of BMD remains the primary tool for fracture risk and osteoporosis treatment assessment, and is the central component of internationally agreed definitions of osteoporosis [31]. An important limitation of the studies identified by this analysis is that no report changes in BMD during or following critical illness. A single study reported an increased in fragility fracture risk in older females following ICU compared to population controls, and although this was a large study with a high methodological quality score, it was limited by its retrospective design [18]. There are no studies reporting the use of bone histomorphometric analysis of bone biopsies or other methods for assessing bone microarchitecture (high-resolution CT or MRI imaging) in critically ill patients. Bone histomorphometry could provide information regarding the effects of critical illness on microarchitectural deterioration, mineralisation and dynamic indices of bone resorption, and formation.
Bone turnover markers were the outcome measured in 10 of the 11 studies identified in this review. BTMs are an important tool to assess progression of osteoporosis, fracture risk, and treatment response [29, 32, 33]. Overall, BTMs are separated into markers of bone resorption (PyD, DpD, B-CTX/ICTP) and bone formation (ALP, BALP, OC, P1CP, P1NP) [34]. However, BTM levels are affected by a number of factors, requiring more complex interpretation. Osteocalcin is a marker of osteoblast function and bone formation, but smaller fragments are derivatives of bone resorption and included in assay. The bone formation markers P1NP and P1CP are both procollagen terminal extension peptides, but P1NP is more specific for bone formation. Also, a number of BTMs are affected by biological factors including age, gender, co-existing disease, and medications [34]. Examples include decreased excretion of B-CTX in renal failure [34] and sensitivity of OC to glucocorticoid exposure [35].
The studies identified in this review consistently described changes in BTMs during critical illness suggestive of an increased osteoclastic bone resorption (increased urinary DpD and PyD, serum B-CTX/ICTP), an increase in immature osteoblast number and activity (serum P1CP and P1NP), and a reduced activity of mature osteoblasts (serum OC and ALP). The increase in bone resorption markers described in these studies is of the magnitude described in postmenopausal females, or metabolic bone disease [33, 36, 37], and has been likened to other metabolic bone disorders, such as Paget’s disease, where uncoupling of bone osteoclast and osteoblast activity is described [26].
A limitation of the studies using BTMs to assess bone turnover in this analysis was the short duration of follow-up, ranging from 1 to 26 days, and a lack of premorbid assessment of bone turnover or skeletal health. When BTMs are used to assess treatment effect of anti-resorptive agents, an interval of 3–6 months is normally recommended [35]. Although these studies are not designed to assess the effect of anti-resorptive agents on bone turnover, the short duration of follow-up decreases the ability to establish a causal relationship between critical illness and bone turnover.
An important limitation of the evidence identified by this review is the limited analysis of the effect of possible confounding variables on the association between critical illness and altered bone turnover. Although six of the studies provided an age- and gender-matched assessment of a control group, the effects of other known causes of osteoporosis and variables, known to affect the metabolism of BTMs (including menopausal status, renal failure, liver disease, diabetes, thyroid disease, and medications) [36, 37], were not consistently addressed. These variables are likely to occur in critically ill patients, leaving the possibility that altered metabolism of BTMs or known risk factors for osteoporosis are partly or wholly responsible for the observed increase in bone turnover.
The studies in this analysis do provide some information about the relationship between critical illness duration, inflammation, immunomodulation, endocrine dysfunction, and increased bone turnover. Higher levels of bone resorption markers were observed in ICU patients with a length of stay of greater than 5 days compared to less than 5 days [28]. This may indicate a relationship between duration of critical illness and bone resorption, although the lack of adjustment for confounders, including co-morbid illness such as renal failure, prevents the nature of this relationship being established.
Vitamin D deficiency with resultant secondary hyperparathyroidism and prolonged immobilisation may increase the risk of excessive bone resorption; however, a range of metabolic abnormalities characterised as primary hyperparathyroidism, secondary hyperparathyroidism, and mixed disorder were described in critically ill patients with elevated bone resorption markers [19]. Two studies report the effects on bone turnover of treating vitamin D deficiency in critically ill patients. The interventional data from one study in this analysis described the effect of parenteral vitamin D 200 IU or 500 IU daily in long-term surgical ICU patients receiving parenteral nutrition. Higher dose vitamin D was associated with a relatively small increase in serum OC, and a decrease in serum B-CTX, but did not affect other BTMs. In addition, the decrease in inflammatory markers interleukin-6 and C-reactive protein over time was more pronounced with the higher dose vitamin D [26]. However, treating vitamin D deficiency with calcitriol did not lead to a reduction in bone resorption markers, suggesting that vitamin D deficiency was not the mechanism for accelerated bone turnover [21].
A positive relationship between inflammation and increased bone turnover was present in a number of studies [22–24, 26], and was unrelated to severity of illness, type of illness, age, or outcome [26]. Systemic inflammation has been identified as a marker for increased fracture risk in non-critically ill patients, with a 23 % increase risk of fracture associated with each standard deviation increase in the inflammatory marker high-sensitivity C-reactive protein [38]. Inflammatory cytokines such as TNF-α and IL-6 are potent stimulators of RANK ligand-mediated activation of osteoclastogenesis and direct activation of osteoclast precursors [26]. Ongoing bone resorption did not correlate with inflammatory markers, which may reflect the influence of other mechanisms, a prolonged effect of cytokines through osteoclast activation factors that increases maturation and lifespan of osteoclasts, or a direct effect of cytokines on osteoclast precursors. In one of the studies, concomitant treatment with glucocorticoids, thyroid hormones, or any other ICU medication did not significantly affect markers of bone turnover at any of the studied time points [26].
A series of studies included in this review by Van den Berghe et al. [22–24] described changes to the somatotrophic, thyrotrophic, and gonadotrophic axes in prolonged critical illness, and included bone markers as a part of measures of target tissue effects. The studies describe a positive correlation between inflammatory cytokines and osteoclastic and osteoblastic activity, with variable effects of restoration of somatotrophic, thyrotrophic, and gonadotrophic axes on BTMs. The administration of growth hormone-releasing peptide (GHRP) alone led to reactivation of pulsatile GH secretion in critically ill patients, but no changes in BTMs [22]. The addition of thyroid releasing hormone (TRH) led to increased osteocalcin, suggesting impaired maturation of osteoblasts may be explained by a suppressed thyroid axis [22]. Finally, the addition of gonadotropin-releasing hormone (GnRH) led to a further increase in osteocalcin [22, 23]. This complex relationship between sex hormones and altered bone turnover markers in critical illness is not surprising given the increasingly complicated interaction between these regulators of osteoclast differentiation and activity [39].
In vitro experiments have shown that compared to healthy controls, critically ill patients’ peripheral blood mononuclear cells (PBMCs) responded to the presence of osteoclastic activation factors with an increased number and activity of mature osteoclasts [25]. In addition, exposure of PBMCs to critically ill patient sera resulted in an increased formation of mature osteoclasts, whereas a model of bone formation showed a reduction in angiogenesis factor expression, and reduced vascularity and maturity of bone formation.
This systematic review provides moderate evidence of a relationship between critical illness and increased bone turnover. Increased bone turnover may lead to impaired fracture healing or post-ICU fragility fractures, with their associated morbidity and mortality. Increased bone turnover is associated with mortality in elderly patients [40] and patients with cardiovascular disease [41]. If future studies find that survivors of critical illness are at high risk of subsequent fragility fracture, target interventions to prevent or attenuate acute bone loss such as the early administration of anti-resorptive therapies may be assessed as a broader fracture prevention strategy.
There is limited evidence examining the efficacy of bisphosphonates in this setting. A randomised controlled trial identified in the search strategy and excluded from this analysis reported a transient decrease in serum B-CTX in chronic critically ill patients receiving a single intravenous dose of ibandronate compared to placebo [42]. In addition, the decrease in the bone turnover marker (serum OC) observed in postmenopausal women receiving ibandronate [43] was not observed in this study, supporting the theory that bone formation and resorption is uncoupled in critical illness. Although limited by small sample size, short follow-up, and limited extent and duration of effect, this study provides evidence that suppression of excessive bone resorption in critical illness is possible.
The higher-quality cohort and case–control studies provide moderate evidence for an association between critical illness requiring intensive care admission, and increased bone turnover. A prospective observational study evaluating BMD changes in the year after critical illness, with comparisons to age- and gender-matched population controls, and adjustment for known risk factors and possible critical illness factors is now required.
References
Cuthbertson BH, Scott JE, Strachan M, Kilonzo M, Vale L (2005) Quality of life before and after intensive care. Anaesthesia 60:332–339
Niskanen M, Ruokonen E, Takala J, Rissanen P, Kari A (1999) Quality of life after prolonged intensive care. Crit Care Med 27:1132–1139
Herridge MS, Cheung AM, Tansey CM et al (2003) One-year outcome in survivors of the acute respiratory distress syndrome. N Engl J Med 348(8):683–693
Chelluri L, Pinsky MR, Donahoe MP, Grenvik A (1993) Long-term outcome of critically ill elderly patients requiring intensive care. JAMA 269(24):3119–3123
Dowdy DW, Eid MP, Sedrakyan A et al (2005) Quality of life in adult survivors of critical illness: a systematic review of the literature. Intensive Care Med 31(7):1007
Angus DC, Carlet J (2003) Surviving intensive care: a report from the 2002 Brussels Roundtable. Intensive Care Med 29(3):368–377
Douglas SL, Daly BJ, Kelley CG, O’Toole E, Montenegro H (2005) Impact of a disease management program upon caregivers of chronically critically ill patients. Chest 128(6):3925–3936
Nguyen TV, Center JR, Eisman JA (2004) Osteoporosis: underrated, underdiagnosed and undertreated. MJA 180:S18–S22
Seeman E (2002) Pathogenesis of bone fragility in women and men. Lancet 359:1841–1850
Andrade SE, Majumdar SR, Chan A et al (2003) Low frequency of treatment of osteoporosis among postmenopausal women following a fracture. Arch Intern Med 163:2052–2057
Vestergaard P, Rejnmark L, Mosekilde L (2005) Osteoporosis is markedly underdiagnosed: a nationwide study from Denmark. Osteoporos Int 16(2):134–141
Griffith DM, Walsh TS (2011) Bone loss during critical illness: a skeleton in the closet for the intensive care unit survivor? Crit Care Med 39(6):1554–1556
Via MA, Gallagher EJ, Mechanick JI (2010) Bone physiology and therapeutics in chronic critical illness. Ann N Y Acad Sci 1211:85–94
Hollander JM, Mechanick JI (2009) Bisphosphonates and metabolic bone disease in the ICU. Curr Opin Clin Nutr Metab Care 12(2):190–195
Lievense AM, Bierma-Zeinstra SMA, Verhagen AP, Van Baar ME, Verhaar JAN, Koes BW (2002) Influence of obesity on the development of osteoarthritis of the hip: a systematic review. Rheumatology 41:1155–1162
Brennan SL, Pasco JA, Urquhart DM, Oldenburg B, Wang Y, Wluka AE (2010) Association between socioeconomic status and bone mineral density in adults: a systematic review. Osteoporos Int 22(2):517–527
Chalmers TC, Smith H, Blackburn B et al (1981) A method for assessing the quality of a randomized control trial. Control Clin Trials 2:31–39
Orford NR, Saunders K, Merriman E et al (2011) Skeletal morbidity among survivors of critical illness. Crit Care Med 39(6):1295–1300
Nierman DM, Mechanick JI (1998) Bone hyperresorption is prevalent in chronically critically ill patients. Chest 114(4):1122–1128
Lind L, Carlstedt F, Rastad J et al (2000) Hypocalcemia and parathyroid hormone secretion in critically ill patients. Crit Care Med 28(1):93–99
Nierman DM, Mechanick JI (2000) Biochemical response to treatment of bone hyperresorption in chronically critically ill patients. Chest 118(3):761–766
Van den Berghe G, Baxter RC, Weekers F et al (2002) The combined administration of GH-releasing peptide-2 (GHRP-2), TRH and GnRH to men with prolonged critical illness evokes superior endocrine and metabolic effects compared to treatment with GHRP-2 alone. Clin Endocrinol (Oxford) 56(5):655–669
Van den Berghe G, Weekers F, Baxter RC et al (2001) Five-day pulsatile gonadotropin-releasing hormone administration unveils combined hypothalamic-pituitary-gonadal defects underlying profound hypoandrogenism in men with prolonged critical illness. J Clin Endocrinol Metab 86(7):3217–3226
Van den Berghe G, Wouters P, Weekers F et al (1999) Reactivation of pituitary hormone release and metabolic improvement by infusion of growth hormone-releasing peptide and thyrotropin-releasing hormone in patients with protracted critical illness. J Clin Endocrinol Metab 84:1311–1323
Owen HC, Vanhees I, Solie L et al (2012) Critical illness-related bone loss is associated with osteoclastic and angiogenic abnormalities. J Bone Miner Res 27(7):1541–1552
Van den Berghe G, Roosbroeck DV, Vanhove P, Wouters PJ, De Pourcq L, Bouillon R (2003) Bone turnover in prolonged critical illness: effect of vitamin D. J Clin Endocrinol Metab 88(10):4623–4632
Smith LM, Cuthbertson B, Harvie J, Webster N, Robins S, Ralston SH (2002) Increased bone resorption in the critically ill: association with sepsis and increased nitric oxide production. Crit Care Med 30(4):837–840
Shapses SA, Weissman C, Seibel MJ, Chowdhury HA (1997) Urinary pyridinium cross-link excretion is increased in critically ill surgical patients. Crit Care Med 25(1):85–90
Vasikaran S, Eastell R, Bruyère O et al (2011) Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: a need for international reference standards. Osteoporos Int 22(2):391–420
Mechanick JI, Brett EM (2002) Endocrine and metabolic issues in the management of the chronically critically ill patient. Crit Care Clin 18(3):619–641
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359:1929–1936
Tamaki J, Iki M, Kadowaki E et al (2013) Biochemical markers for bone turnover predict risk of vertebral fractures in postmenopausal women over 10 years: the Japanese Population-based Osteoporosis (JPOS) Cohort Study. Osteoporos Int 24(3):887–897
Nishizawa Y, Ohta H, Miura M et al (2012) Guidelines for the use of bone metabolic markers in the diagnosis and treatment of osteoporosis (2012 edition). J Bone Miner Metab 31(1):1–15
Hlaing TT, Compston JE (2014) Biochemical markers of bone turnover—uses and limitations. Ann Clin Biochem 51:189–202
Kotowicz MA, Hall S, Hunder GG et al (1990) Relationship of glucocorticoid dosage to serum bone Gla-protein concentration in patients with rheumatologic disorders. Arthritis Rheum 33(10):1487–1492
Seibel MJ, Eastell R, Garnero P, Stepan J (2000) The use of biochemical markers of bone turnover in osteoporosis. Osteoporos Int 11(suppl 6):S2–S17
Vasikaran S, Cooper C, Eastell R et al (2011) International Osteoporosis Foundation and International Federation of Clinical Chemistry and Laboratory Medicine position on bone marker standards in osteoporosis. Clin Chem Lab Med 49(8):1271–1274
Pasco JA, Kotowicz MA, Henry MJ et al (2006) High-sensitivity C-reactive protein and fracture risk in elderly women. JAMA 296(11):1353–1354
Frenkel B, Hong A, Baniwal SK et al (2010) Regulation of adult bone turnover by sex steroids. J Cell Physiol 224:305–310
Sambrook PN, Chen CJ, March L et al (2006) High bone turnover is an independent predictor of mortality in the frail elderly. J Bone Miner Res 21(4):549–555
Lerchbaum E, Schwetz V, Pilz S et al (2013) Association of bone turnover markers with mortality in men referred to coronary angiography. Osteoporos Int 24(4):1321–1332
Via MA, Potenza MV, Hollander J et al (2012) Intravenous ibandronate acutely reduces bone hyperresorption in chronic critical illness. J Intensive Care Med 27(5):312–318
Delmas PD, Adami S, Strugala C et al (2006) Intravenous ibandronate injections in postmenopausal women with osteoporosis: one-year results from the dosing intravenous administration study. Arthritis Rheum 54(6):1838–1846
Acknowledgments
SLB is supported by the NHMRC Early Career Fellowship (1012472).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Orford, N., Cattigan, C., Brennan, S.L. et al. The association between critical illness and changes in bone turnover in adults: a systematic review. Osteoporos Int 25, 2335–2346 (2014). https://doi.org/10.1007/s00198-014-2734-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2734-1